Optimizing Contraception for Women with HIV
The ideal contraceptive for a woman with HIV will help prevent pregnancy as well as the transmission of HIV and STIs. Dual contraception using condoms plus an additional contraceptive is the best strategy. Preexposure (PrEP) and postexposure (PEP) prophylaxis should be available to partners regardless of contraceptive method used.
The NIH states
Women with HIV can use all available contraceptive methods (e.g., pill, patch, ring, injection, implant) and intrauterine devices (IUDs) after consideration of potential drug–drug interactions
SUMMARY:
- Combined hormonal contraception (pill, patch and ring & LARC) and progestin-only pills can be used in women with HIV
- Drug-drug interactions: Antiretroviral (ARV) drugs
- Interactions between hormonal contraception and ARV drugs can reduce contraceptive efficacy | Data is limited
- Concern for ARV drug interactions should not prevent offering hormonal contraceptives for patients
- HIV.gov (NIH) provides tables to assist in determining risk for significant drug-drug interactions (see ‘Learn More – Primary Sources’ below)
- Alternative or additional contraception should be used if significant interactions may occur
- Combination contraceptives containing ethinyl estradiol and progestins (combined oral contraceptives, transdermal patches, and intravaginal rings)
- Can decrease hormone levels but are still considered safe (either CDC Medical Eligibility Criteria (MEC) 1 or 2 depending on which antiretroviral is being used)
- Protease inhibitors, pharmacologic boosters, and efavirenz can cause decreased effectiveness of hormonal contraception
- Fostemsavir: can cause increased levels of ethinyl estradiol and raise risk of thromboembolic events | Dosing of ethinyl estradiol should not be higher than 30 mcg daily
- Progestin-only pills
- Efavirenz can cause decreased effectiveness of hormonal contraception by lowering progestin concentrations
- May impact emergency contraception as well, increasing risk of failure
- Contraceptive implants
- Are highly effective and benefits outweigh risks in women with HIV (MEC 1)
- Injectable depot medroxyprogesterone acetate (DMPA) is safe and effective (MEC 1) and does not appear to have interactions with antiretrovirals
- Intrauterine devices, both copper containing and levonorgestrel-releasing
- MEC 1 for women with HIV who are clinically well and on antiretrovirals, with no known drug interactions with antiretrovirals
- For women with HIV who are not clinically well or not on antiretrovirals, initiation of IUD is considered MEC 2, but continuation for an already placed IUD is 1
- Limited data suggest a low risk of pelvic inflammatory disease and no changes in genital shedding of HIV RNA
- Condoms reduce transmission of HIV between discordant partners but are not represent optimal contraception, with an annual pregnancy rate of over 15% per year. Should be used concurrently with another contraceptive method
- Spermicides: not recommended due to potential of causing genital lesions
- Nonoxynol-9, the active ingredient in most formulations, can cause genital lesions and may increase the likelihood of HIV transmission to a partner
KEY POINTS:
- HIV infection does not pose a barrier to sterilization, which remains an appropriate contraceptive option
- Emergency contraception including hormone-based (progestin-only pills, ulipristal acetate, combined oral contraceptives), and the copper IUD should be offered to women with HIV whenever appropriate
- Spermicides are not recommended
- CDC US MEC Categories of medical eligibility criteria for contraceptive use
- MEC 1 = A condition for which there is no restriction for the use of the contraceptive method
- MEC 2 = A condition for which the advantages of using the method generally outweigh the theoretical or proven risk
- MEC 3 = A condition for which the theoretical or proven risks usually outweigh the advantages of using the method
- MEC 4 = A condition that represents an unacceptable health risk if the contraceptive method is used
Learn More – Primary Sources:
CDC (MMWR) United States medical eligibility criteria for contraceptive use, 2024
U.S. MEC and U.S. SPR Provider Tools | Contraception | CDC
NIH: Antiretroviral medication Fostemsavir (FTR, Rukobia)
Contraception: Contraceptive failure in the United States

Syphilis: CDC Diagnosis and Treatment Guidelines
WHAT IS IT?
Syphilis is a sexually transmitted infection caused by Treponema pallidum. Symptoms, diagnostic tests and treatment vary depending on stage of the disease. The syphilis rates in the US have continued to rise over the past decade. Without treatment, syphilis can damage the brain, nerves, eyes, and cardiovascular system.
Screening for Syphilis
Who to Screen
- The USPSTF task force recommends screening for the following populations (Grade A recommendation: “Offer or provide this service”)
- Asymptomatic, nonpregnant adolescents and adults who are at increased risk for syphilis infection
- All pregnant women early in pregnancy
- Factors associated with increased risk for syphilis include
- Higher prevalence of infection in particular communities
- Sociodemographic and behavioral factors (e.g., multiple sex partners, prevalence of syphilis is higher in males, men who have sex with men, drug use, persons living with HIV, young adults, and persons with a history of incarceration, sex work, or military service)
How to Screen
- Traditional screening: Initial “nontreponemal” antibody test (i.e., Venereal Disease Research Laboratory [VDRL] test or rapid plasma reagin [RPR] test) to detect biomarkers released from damage caused by syphilis infection, followed by a confirmatory “treponemal” antibody detection test (i.e., fluorescent treponemal antibody absorption [FTA-ABS] or T pallidum particle agglutination test [TP-PA])
- Reverse sequence screening algorithm: Automated treponemal test (such as an enzyme-linked [EIA], chemiluminescence [CIA], or multiplex flow immunoassay [immunoblot]) performed first, followed by a nontreponemal test
- If the test results of the reverse sequence algorithm are discordant, a second treponemal test (preferably using a different treponemal antibody) is performed
Primary Syphilis
Early disease, characterized by an ulcer or chancre at the infection site approximately 3 weeks after infection
- Diagnosis
- Darkfield examination and molecular tests of fluid/tissue for T. pallidum are definitive methods or
- Presumptive diagnosis requires both a (1) nontreponemal test (VDRL or RPR) and (2) a treponemal test (FTA-ABS, EIA, CIAs and immunoblots, rapid treponemal tests or TP-PA)
- Treatment
- Benzathine penicillin G 2.4 million units IM in a single dose
Secondary Syphilis
Symptoms can be diffuse and variable
- Symptoms
- Skin rash ucocutaneous lesions Lymphadenopathyn Fever
- Typically develops several weeks to months after primary infection
- Diagnosis
- Same as for primary syphilis
- Treatment
- Same as for primary syphilis
Latent Syphilis
No symptoms and no current evidence of primary, secondary, or tertiary disease
- Diagnosis of early latent syphilis
- Documented seroconversion or sustained ( >2 weeks) fourfold or greater increase in nontreponemal test or unequivocal symptoms of primary/secondary syphilis or a sex partner with documented primary/secondary syphilis all within the past year
- Treatment
- Early latent (acquired within 1 yr): Benzathine penicillin G 2.4 million units IM single dose
- Late latent (acquired > 1 yr): Benzathine penicillin G 7.2 million units total given IM in 3 weekly doses of 2.4 million units each
Tertiary Syphilis
Gummas, cardiovascular syphilis (CNS involvement (for neurosyphilis treatment, see below)
- Diagnosis
- Appearance of soft skin lesions and ulcers
- CXR shows linear calcifications of aorta
- Perform LP to rule out neurosyphilis
- Treatment
- Benzathine penicillin G 7.2 million units administered as 3 weekly doses of 2.4 million units
Neurosyphilis
Note: Can occur at any stage | Includes cranial nerve dysfunction, meningitis, stroke, altered mental status, auditory/ophthalmic abnormalities | Tabes dorsalis and paresis are late manifestations and can occur 10 to 30 years after infection
- Diagnosis
- Lumbar puncture: Test CSF for white blood cell count, protein and VDRL
- Treatment
- Aqueous crystalline penicillin G, 3 to 4 million units IV every 4 hours for 10 to 14 days or penicillin G procaine, 2.4 million units IM daily plus probenicid 500 mg orally 4 times daily, for 10 to 14 days
Note: The durations of the recommended and alternative regimens for neurosyphilis are shorter than the duration of the regimen used for latent syphilis | Therefore, benzathine penicillin, 2.4 million units IM once per week for 1 to 3 weeks, can be considered after completion of these neurosyphilis treatment regimens to provide a comparable total duration of therapy
KEY CLINICAL POINTS:
- Penicillin Allergy
- Patients with penicillin allergy should be desensitized and treated with penicillin whenever possible
- Doxycycline 100 mg BID x 14 days or tetracycline 500 mg 4 times daily for 14 days can be used for nonpregnant penicillin-allergic patients with primary or secondary syphilis
- Counsel patients regarding Jarisch-Herxheimer reaction
- Acute febrile reaction frequently accompanied by headache, myalgia, and fever
- Occurs within initial 24 hours after initiation of any syphilis therapy
- Reaction to treatment and not an allergic reaction to penicillin
- Occurs most frequently among persons who have early syphilis (likely due to heavier bacterial loads at this stage)
- Manage with antipyretics
- Nontreponemal titers decline after treatment and eventually become negative
- Treponemal tests remain positive for life
- Follow-up at
- 6, 12, 18 and 24 months after therapy and should include serology
- If symptoms persist or recur, or there is a >4 fold increase in nontreponemal test titer persisting more than 2 weeks
- consider reinfection or treatment failure
- retreat and check HIV status
- Sexual transmission occurs only when mucocutaneous lesions are present and is uncommon after the first year
- Persons exposed sexually to those with primary, secondary or early latent syphilis should be evaluated clinically and serologically
Learn More – Primary Sources:
USPSTF: Screening for Syphilis Infection in Pregnant Women
USPSTF: Screening for Syphilis Infection in Nonpregnant Adolescents and Adults
CDC Sexually Transmitted Diseases: Syphilis
CDC: Syphilis During Pregnancy Treatment Guidelines
BMJ Clinical Updates: Syphilis
CDC (MMWR): Missed Opportunities for Preventing Congenital Syphilis — United States, 2022
Sexually Transmitted Infections and Partner Notification
The sex partners of persons with sexually transmitted infections (STIs) require treatment. This treatment has been a central component of prevention and control of bacterial STIs in the United States for decades. Traditionally, it has been left to patients or health care providers to notify partners of infected persons of their exposure to an STI. Common practice is to inform, evaluate and treat sex partners of persons infected with STIs. Partner management arose from the campaign to control syphilis and ultimately, congenital syphilis. Now partner management has become widely recommended for gonorrhea, chlamydial infection and, most recently, human immunodeficiency virus (HIV) infection. However, for STIs other than syphilis, partner management based on provider referral is rarely assured, while patient referral has had only modest success in assuring partner treatment.
An alternative approach to assuring treatment of partners is expedited partner therapy (EPT). EPT is the delivery of medications or prescriptions by persons infected with an STI to their sex partners without clinical assessment of the partners. Clinicians ranging from physicians to public health workers give the infected persons sufficient medications directly or a prescription for the patients and their partners. Following an evaluation of medical studies on EPT, the CDC concluded that EPT is a “useful option” to further partner treatment, particularly for male partners of women with chlamydia or gonorrhea. CDC addresses this practice for certain populations and specific conditions.
Throughout discussions of EPT, the legal status of the practice remained a gray area. Therefore, CDC collaborated with two public health centers to assess the legal framework concerning EPT across all 50 states and other jurisdictions (the District of Columbia and Puerto Rico). Assessment of local statutes excluding the District of Columbia and tribal laws for sovereign nations was not undertaken.
The CDC’s EPT Legal Status color-coded map (see ‘Learn More – Primary Sources’ below) shows the states and jurisdictions where EPT is allowable or potentially allowable. Of note, this map also shows those states where EPT is prohibited. The most cited reason is that a physician patient relationship is required. The relationship could require a physical exam, discussion with the patient, or availability for follow-up.
ACOG Recommendations
- ACOG supports EPT to prevent gonorrhea and chlamydial reinfection
- Committee Opinion updated to include the possible role of EPT for trichomoniasis (although no particular management approach appears superior)
- Members of ACOG should advocate to legalize EPT
- The Committee Opinion states
Expedited partner therapy is recommended only after an obstetrician–gynecologist or other provider has assessed the risk of intimate partner violence associated with partner notification. It is not intended for use in cases of suspected child abuse, sexual assault, or any other situation in which the patient’s safety from her abuser may be compromised.
Learn More – Primary Sources:
CDC Expedited Partner Therapy
ACOG Committee Opinion 737: Expedited Partner Therapy
Color-coded map: Legal Status of Expedited Partner Therapy (EPT)
A Review of Expedited Partner Therapy for the Management of Sexually Transmitted Infections in Adolescents
Perspectives on expedited partner therapy for chlamydia: a survey of health care providers.
Expedited Partner Therapy: Clinical Considerations and Public Health Explorations
Patient-Delivered Partner Therapy (PDPT) for Chlamydia, Gonorrhea, and Trichomoniasis: Guidance for Medical Providers in California (sample EPT regimens)
Screening & Treatment of Gynecologic infections in the HIV-Positive Woman
Gynecologic infections are more common, and may be more difficult to eradicate, in the HIV population. Overall, treatment protocols remain the same, irrespective of HIV status, although there are some differences depending on the disorder.
CLINICAL ACTIONS:
- Screen at entry to care and at least annually for the following: N. gonorrhoeae, C. trachomatis, syphilis and vaginal trichomoniasis
- Screen for hepatitis C on entry to care
- At-risk seronegative individuals should be screened at least annually
- Consider type specific HSV serologic testing for those presenting for an STD evaluation
- Approximately 70% of persons with HIV are HSV-2 seropositive | 95% are seropositive for either HSV-1 or HSV-2
- HSV-2 infection increases the risk of HIV acquisition two- to three-fold and in coinfected patients
- HSV-2 reactivation results in increases in HIV RNA levels in blood and genital secretions
- Screen on entry to care for hepatitis B with HBsAg, anti-HBc and/or anti-HBs
- Offer vaccination to seronegative individuals with hepatitis B or combined hepatitis A and B vaccine
- Recheck immunity after vaccination complete
SYNOPSIS:
While it is critical to remain vigilant with regard to STDs and pelvic infections, women with ulcerative conditions of the genitalia, including syphilis and herpes, are at increased risk of HIV acquisition and transmission to partners, lending an urgency to prompt treatment or suppression (see separate entry on ulcerative conditions).
KEY POINTS:
- Bacterial vaginosis is more prevalent/persistent in HIV-positive women
- Diagnosis and treatment options are the same
- Vulvovaginal candidiasis is more common among HIV-positive women and associated with decreased CD4+ counts
- Treatment is the same as for HIV-negative women
- For azole-refractory Candida glabrata vaginitis
- Boric acid 600 mg vaginal suppository once daily for 14 days
- Note: Severe or recurrent vaginitis should be treated with oral fluconazole (100 to 200 mg) or topical antifungals for ≥7 days
- Treatment for gonorrhea/chlamydia is the same as for HIV-negative women
- Retest 3 months after treatment as reinfection is common
- Pelvic inflammatory disease is treated with the same antimicrobials for the same duration as for HIV-negative
- There is a greater incidence of tubo-ovarian abscess among HIV-positive, but overall response to therapy is the same as for HIV-negative
- Trichomoniasis is more prevalent among HIV-positive and should be treated with a one week course of metronidazole
- Parasitic conditions such as scabies or pediculosis pubis are treated the same regardless of HIV status
Learn More – Primary Sources:
ACOG Practice Bulletin 167: Gynecologic Care for Women and Adolescents with Human Immunodeficiency Virus
NIH Guidelines for Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents
CDC: Sexually Transmitted Infections Treatment Guidelines 2021
Ulcerative Genital Conditions in the HIV-Positive Woman
Genital, anal, or perianal ulcers are generally caused by syphilis or herpes. Chancroid, lymphogranuloma venereum (LGV), and granuloma inguinale (donovaniasis) are less likely diagnoses; however, all these conditions are associated with increased HIV acquisition and transmission. Guidelines for screening and treatment differ in some cases from those for the HIV-negative patient.
CLINICAL ACTIONS:
- Evaluate first for herpes and syphilis first
- Other causes such as chancroid and lymphogranuloma venereum should then be considered
Herpes Simplex (HSV)
Syphilis
Chancroid
Lymphogranuloma Venereum (LGV)
Granuloma Inguinale (donovaniasis)
Herpes Simplex lesions:
- Caused by herpes simplex viruses (HSV)
- Common and may be severe, painful and atypical
- Offer HSV type-specific serologic testing on initial HIV evaluation for asymptomatic individuals
- HSV DNA polymerase chain reaction (PCR) and viral culture are preferred methods for diagnosis of mucocutaneous HSV lesions caused by HSV
- Consider suppression or episodic therapy to decrease clinical manifestations if HSV-2 is detected
- Does not reduce risk for HIV transmission or HSV-2 transmission to susceptible sex partners
- Generally higher doses/longer duration of treatment are recommended for HIV-positive women
Daily suppression
- Acyclovir 400-800 mg BID or TID
or
or
Episodic flares
- Acyclovir 400 mg TID x 5-10 days
or
- Valacyclovir 1 g BID x 5-10 days
or
- Famcycolovir 500 mg BID x 5-10 days
Syphilis:
- Systemic disease caused by Tremonema Pallidum
- Primary syphilis is characterized by genital ulcers, though secondary/ tertiary/latent forms are not
- A presumptive diagnosis of syphilis requires a treponemal test (i.e fluorescent treponemal antibody absorbed tests [FTA-ABS]) plus a nontreponemal test (i.e. Venereal Disease Research Laboratory [VDRL] or Rapid Plasma Reagin [RPR])
- Screen for syphilis on initial HIV evaluation and annually thereafter
- Treatment is the same regardless of HIV status
- Penicillin G IM is the preferred treatment for all stages; the preparation (benzathine, aqueous procaine aqueous crystalline), dosage and length of treatment depend on the stage
Chancroid:
- Painful, genital ulcers with suppurative lymphadenopathy caused by ducreyi
- Treatment is the same regardless of HIV status
- Close follow up is required as treatment failure is increased in the HIV positive
Treatment
or
or
- Ciprofloxacin 500 mg po BID x 3 days
or
- Erythromycin 500 mg tid x 7 days
Lymphogranuloma Venereum (LGV)
- Tender, unilateral groin/femoral lymphadenopathy with a self-limited genital ulcer/papule caused by C. trachomatis serovars L1, L2, or L3
- Proctitis may occur
- Diagnose by identifying C. trachomatis from the lesion by culture, direct immunofluorescence or nucleic acid detection
- Treatment is the same regardless of HIV status
Treatment
- Doxycycline 100 mg BID x 3 weeks
or
- Erythromycin base 500 mg QID x 3 weeks
Granuloma Inguinale (Donovanosis):
- Painless ulcerative disease characterized by beefy red, highly vascular lesions caused by Klebsiella granulomatis
- Diagnose by identifying dark-staining “Donovan Bodies” on biopsy or tissue
- Treatment is the same regardless of HIV status
Treatment
- Azithromycin 1 gm once/week or 500 mg/day x 3 weeks/until lesions healed
or
- Doxycycline 100 mg BID X 3 weeks/until lesions healed
or
- Ciprofloxacin 750 mg BID x 3 weeks/until lesions healed
or
- Erythromycin base 500 mg QID x 3 weeks/until lesions healed
or
- Trimethoprim-sulfamethoxazole double strength BID x 3 weeks/until healed
SYNOPSIS:
Vaginal, vulvar, and sexually transmitted infections may increase the risk of HIV transmission. Prompt diagnosis and treatment decreases the likelihood of transmission; public health standards require providers to presumptively treat any patient, regardless of HIV status, with suspected syphilis immediately and before test results are available. Presumptive treatment of primary herpes is also recommended as early treatment maximizes success.
KEY POINTS:
- Genital, anal, or perianal lesions may not necessarily be infectious (e.g. trauma, carcinoma, aphthous, drug eruption, psoriasis)
- Medical history and physical exam findings are frequently inaccurate and should be followed by tests that reflect conditions prevalent in the area
- Consider biopsy for ulcers not responding to therapy or if the diagnosis is unclear
- If HIV status is unknown, HIV testing should be offered to any woman with genital/anal ulcers presenting for treatment.
Diagnosis codes:
- D28.9 benign neoplasm of female genital organs, unspecified
- Z21 HIV infection
Learn More – Primary Sources:
2015 Sexually Transmitted Disease Treatment Guidelines
ACOG Practice Bulletin 167: Gynecologic Care for Women and Adolescents with Human Immunodeficiency Virus
NIH Guidelines for Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents
Trichomoniasis: CDC Diagnosis and Treatment Guidelines
SYNOPSIS:
Trichomoniasis is the most prevalent nonviral sexually transmitted infection worldwide. The U.S. population-based T. vaginalis prevalence is 2.1% among females and 0.5% among males, with the highest rates among Black females (9.6%) and Black males (3.6%), compared with non-Hispanic White women (0.8%) and Hispanic women (1.4%) The majority of persons who have trichomoniasis (70%–85%) either have minimal or no genital symptoms, and untreated infections might last from months to years, however, data are lacking on whether screening and treatment for asymptomatic trichomoniasis is beneficial. Decisions about screening might be informed by local epidemiology of T. vaginalis infection rates.
CLINICAL ACTIONS:
Male: Urethritis| Epididymitis | Prostatitis
Women: Vaginal Discharge| Vulvar Irritation
Diagnostic testing for T. vaginalis should be performed in women seeking care for vaginal discharge (yellow-green, with or without irritation). Screening might be considered for women receiving care in high-prevalence settings.
Diagnosis
- Perform nucleic acid amplification testing (NAAT), which detects T. vaginalis genetic material, is highly sensitive and which is three to five times more likely to identify T. vaginalis infections than wet-mount microscopy, a method with poor sensitivity
- Culture was considered the gold standard before molecular testing and is less sensitive than newer tests
- If wet preparations are used, despite lower sensitivities, slides should be evaluated immediately as sensitivity declines with time
- If negative, consider follow up with a NAAT to make sure infection is truly not present
- T. vaginalis may be an incidental finding on a Pap test, neither conventional nor liquid-based Pap tests are considered diagnostic tests for Trichomoniasis, because false negatives and false positives can occur
KEY POINTS:
The nitroimidazoles are the only class of antimicrobial medications known to be effective against T. vaginalis infections. Of these drugs, metronidazole and tinidazole have been cleared by FDA for the oral or parenteral treatment of trichomoniasis.
The CDC recommends the following
- Women
- Metronidazole 500 mg 2 times/day for 7 days
- Men
- Metronidazole 2 g orally in a single dose
- Alternative regimen for men and women
- Tinidazole 2 g orally in a single dose
Note: ACOG also recommends metronidazole 500 mg orally twice a day for 7 days as the recommended treatment option with tinidazole, 2 g orally in a single dose as the alternative regimen
- Alcohol consumption should be avoided during treatment with nitroimidazoles
- To reduce the possibility of a disulfiram-like reaction, abstinence from alcohol use should continue for 24 hours after completion of metronidazole or 72 hours after completion of tinidazole
- Providers should advise persons infected with T. vaginalis to abstain from sex until they and their sex partners are treated (i.e., when therapy has been completed and any symptoms have resolved)
- Testing for other STDs including HIV should be performed in persons infected with T. vaginalis
- Retest for T. vaginalis is recommended for all sexually active women within 3 months following initial treatment
- Testing by NAAT can be conducted as soon as 2 weeks after treatment
- Treat current partners to avoid reinfection and further transmission
- Partners should be advised to abstain from intercourse until they and their sex partners have been adequately treated and any symptoms have resolved
- In States where legally allowed (see learn more below), consider Expedited Partner Therapy (EPT) which allows the patient herself to provide medications to her partner when there are limited public health services to treat a partner, or concern that the partner will not have access to treatment
Pregnancy
- T. vaginalis infection is associated with two to threefold increased risk for HIV acquisition, preterm birth, and other adverse pregnancy outcomes among pregnant women
- However, some trials have not shown improvement in perinatal morbidity with treatment
- Symptomatic pregnant women, regardless of pregnancy stage, should be tested and considered for treatment with metronidazole
- Tinidazole should be avoided for pregnant women
- The benefit of routine screening for T. vaginalis in asymptomatic pregnant women has not been established
HIV
- Among women with HIV infection, up to 53% are also infected with T. vaginalis which has been associated with an increased risk for PID
- Routine screening of asymptomatic women with HIV infection for T. vaginalis is recommended on entry to care, and then annually
- Pregnant women, including those who are asymptomatic, should be screened and treated as necessary because T. vaginalis infection is a risk factor for vertical HIV transmission
- The recommended regimen in the setting of HIV is as follows
- Metronidazole 500 mg twice daily for 7 days
- Retest in 3 months with NAAT
Learn More – Primary Sources:
CDC: Trichomoniasis Treatment Guidelines
CDC: Trichomoniasis Fact Sheet for Your Patients
CDC: Expedited Partner Therapy
ACOG Practice Bulletin 215: Vaginitis in Nonpregnant Patients
Gonorrhea: CDC Diagnosis and Treatment Guidelines
CLINICAL ACTIONS:
Annual screening for gonococcal infection (GC) (N. gonorrhoeae) is recommended for all sexually active women aged <25 years and for older women at increased risk for infection (e.g., those who have a new sex partner, more than one sex partner, a sex partner with concurrent partners, or a sex partner who has a sexually transmitted infection).
Diagnosis
- Perform nucleic acid amplification testing (NAAT), which detects genetic material of N. gonorrhoeae
- More sensitive than culture
- Faster results than culture
- Easy to obtain from a vaginal swab
- Currently approved for genital (vaginal, endocervical) and urine samples
- Can NOT determine antibiotic resistance
OR
- Culture for N. gonorrhoeae
- Requires endocervical swab, not vaginal
- Available for rectal, oropharyngeal, and conjunctival gonococcal infection
NOTE: Obtain BOTH NAAT and culture in the case of treatment failure to determine bacterial susceptibility to antibiotics
SYNOPSIS:
Specific microbiologic diagnosis of infection with N. gonorrhoeae should be performed in all persons at risk for, or suspected to have, gonorrhea. A specific diagnosis can potentially reduce complications, reinfections, and transmission. The CDC no longer recommends combination therapy for uncomplicated GC
KEY POINTS:
For Uncomplicated Gonococcal Infections of the Cervix, Urethra and Rectum
- <150 kg (300 lb): Ceftriaxone 500 mg IM as a single dose
- ≥150 kg (300 lb): 1 g of IM ceftriaxone
- If chlamydial infection has not been excluded
- Treat for chlamydia with doxycycline 100 mg orally twice daily for 7 days
- During pregnancy, azithromycin 1 g as a single dose is recommended to treat chlamydia
If Ceftriaxone is Unavailable
- Gentamicin 240 mg IM as a single dose plus azithromycin 2 g orally as a single dose or
- Cefixime 800 mg orally as a single dose | If treating with cefixime, and chlamydial infection has not been excluded, providers should treat for chlamydia with doxycycline 100 mg orally twice daily for 7 days | During pregnancy, azithromycin 1 g as a single dose is recommended to treat chlamydia
Uncomplicated Gonococcal Infections of the Pharynx
- <150 kg (300 lb): Ceftriaxone 500 mg IM as a single dose
- ≥150 kg (300 lb): 1 g of IM ceftriaxone
- If chlamydial infection has not been excluded
- Treat for chlamydia with doxycycline 100 mg orally twice daily for 7 days
- During pregnancy, azithromycin 1 g as a single dose is recommended to treat chlamydia
Note: No reliable alternative treatments are available for pharyngeal gonorrhea
Newly Approved Antibiotics
- Gepotidacin (BLUJEPA): Oral tablet
- 3,000 mg (four 750 mg tablets) taken orally, followed by a second dose of 3,000 mg (four 750 mg tablets) approximately 12 hours later
- Zoliflodacin (NUZOLVENCE): Single-dose granules dissolved in water
- Single 3‑gram oral dose (one packet of granules mixed with water; must be taken within 15 minutes of mixing
Key Differences & Mechanisms
- Traditional antibiotics: Kill bacteria by blocking cell wall synthesis
- Gepotidacin & zoliflodacin: Block bacterial DNA replication
- Zoliflodacin
- Part of a new class: spiropyrimidinetriones
- Inhibits type II topoisomerase, essential for bacterial survival and reproduction
- Shown active against multidrug‑resistant N. gonorrhoeae, including
- Ceftriaxone‑resistant strains
- Azithromycin‑resistant strains
- No cross‑resistance with existing antibiotics
- Gepotidacin
- A triazaacenaphthylene antibiotic
- Inhibits DNA replication through
- Distinct binding site
- Novel mechanism of action
- Provides balanced inhibition of two type II topoisomerase enzymes
Additional Notes
- Instruct patient to abstain from sexual activity for 7 days after treatment and until all sex partners are adequately treated (7 days after receiving treatment and resolution of symptoms, if present)
- Test for other STIs, including chlamydia, syphilis and HIV
- A test-of-cure is not needed for persons who receive a diagnosis of uncomplicated urogenital or rectal gonorrhea who are treated with any of the recommended or alternative regimens
- In the case of pharyngeal gonorrhea treated with an alternative regimen, the patient should return 14 days after treatment for a test-of cure using either culture or NAAT
- If NAAT positive, do a confirmatory culture and antimicrobial susceptibility testing
- Retest after 3 months
- Recurrence may not be treatment failure but rather reinfection
- In States where legally allowed (see learn more below), consider Expedited Partner Therapy (EPT) which allows the patient herself to provide medications to her partner when there are limited public health services to treat a partner, or concern that the partner will not have access to treatment
- Treat women with HIV with the same recommended regimen
- Consult infectious disease specialist in case of allergies to cephalosporin
Learn More – Primary Sources:
CDC: Gonococcal Infections in Adolescents and Adults
Update to CDC’s Treatment Guidelines for Gonococcal Infection, 2020
FDA Prescribing Information: BLUJEPA
FDA Prescribiing Information: NUZOLVENCE
Chlamydia: CDC Recommendations for Diagnosis and Treatment
CLINICAL ACTIONS:
Annual screening of all sexually active women aged <25 years for chlamydia is recommended, as is screening of older women at increased risk for infection (e.g., those who have a new sex partner, more than one sex partner, a sex partner with concurrent partners, or a sex partner who has an STD).
To diagnose a chlamydia infection:
- Obtain nucleic acid amplification testing (NAAT), which detects genetic material of C. trachomatis
- Highly sensitive in first-catch urine samples and endocervical or vaginal swabs
- Can be collected by a provider or a self-collected vaginal swab
- Certain NAATs have been FDA-cleared for use on liquid-based cytology specimens (collected for Pap smears), however sensitivity may be lower than swabs
SYNOPSIS:
Chlamydial infection is the most frequently reported infectious disease in the United States, and prevalence is highest in persons aged ≤24 years. Several sequelae can result from C. trachomatis infection in women, the most serious of which include PID (pelvic inflammatory disease), ectopic pregnancy, and infertility. Some women who receive a diagnosis of uncomplicated cervical infection already have subclinical upper-reproductive–tract infection.
KEY POINTS:
Chlamydia treatment should be provided promptly for all persons testing positive for infection; treatment delays have been associated with complications
- Recommended Regimens
- Azithromycin 1 g orally in a single dose or
- Doxycycline 100 mg orally twice a day for 7 days
- Alternative Regimens
- Erythromycin base 500 mg orally four times a day for 7 days or
- Erythromycin ethylsuccinate 800 mg orally four times a day for 7 days or
- Levofloxacin 500 mg orally once daily for 7 days or
- Ofloxacin 300 mg orally twice a day for 7 days
- Routine pharyngeal screening for chlamydia is not recommended, but if C. trachomatis is detected in an oropharyngeal specimen treat with azithromycin or doxycycline
- Directly observe patient receiving therapy when single dose therapy is given
- To minimize disease transmission to sex partners, persons treated for chlamydia should be instructed to abstain from sexual intercourse for 7 days after single-dose therapy or until completion of a 7-day regimen and resolution of symptoms if present
- To minimize risk for reinfection, patients also should be instructed to abstain from sexual intercourse until all of their sex partners are treated
- Persons who receive a diagnosis of chlamydia should be tested for HIV, gonococcal infection, and syphilis
- Test-of-cure to detect therapeutic failure is not advised unless therapeutic adherence is in question, symptoms persist, or reinfection is suspected
- Chlamydial NAATs at <3 weeks after completion of therapy is not recommended because the continued presence of nonviable organisms can lead to false-positive results
- Retest after 3 months
- Recurrence may not be treatment failure but rather reinfection
- In States where legally allowed (see ‘Related OBG Topics’ below), consider Expedited Partner Therapy (EPT) which allows the patient herself to provide medications to her partner when there are limited public health services to treat a partner, or concern that the partner will not have access to treatment
- Treat women with HIV with the same recommended regimen
PREGNANCY AND CHLAMYDIAL INFECTION
Risks in pregnancy include preterm labor, premature rupture of membranes and low birth weight with neonates at risk for conjunctivitis (ophthalmia neonatorum) and pneumonia. It is therefore imperative to screen and treat pregnant women with the following:
- Recommended Regimens
- Azithromycin 1 g orally in a single dose
- Alternative Regimens
- Amoxicillin 500 mg orally three times a day for 7 days or
- Erythromycin base 500 mg orally four times a day for 7 days or
- Erythromycin base 250 mg orally four times a day for 14 days or
- Erythromycin ethylsuccinate 800 mg orally four times a day for 7 days or
- Erythromycin ethylsuccinate 400 mg orally four times a day for 14 days
- Test-of-cure (preferably by NAAT) recommended at 3 to 4 weeks after completion of therapy and again after 3 months
- Diagnosis code: Chlamydia: A74.9 (pregnant) or A56.02 (nonpregnant)
Learn More – Primary Sources:
CDC: Chlamydial Infections in Adolescents and Adults
CDC: Chlamydia Fact Sheet for Your Patients
Bacterial Vaginosis – CDC Diagnosis and Treatment Recommendations
CLINICAL ACTIONS:
Bacterial Vaginosis (BV) occurs when normal hydrogen peroxide producing Lactobacillus sp. is replaced by an overgrowth of facultative anaerobic bacteria. If a woman presents with symptoms, including vaginal discharge, irritation and malodor
- Diagnose BV if 3 of the following (Amsel) clinical criteria are present
- Homogeneous, thin, white discharge that smoothly coats the vaginal walls
- More than 20% clue cells (e.g., vaginal epithelial cells studded with adherent coccobacilli) on saline microscopic examination
- pH of vaginal fluid >4.5
- Fishy odor of vaginal discharge before or after addition of 10% KOH (i.e., the whiff test), OR
- Gram stain with Nugent scoring is considered the gold standard to diagnose
-
- Used in research settings; impractical for clinicians so Amsel criteria preferred clinically
- Assigns a score to various bacterial concentrations seen on gram stain: 0-3 Normal | 4-6 Intermediate | 7-10 Bacterial vaginosis
- Affirm VP III (Becton Dickinson, Sparks, MD), a DNA hybridization probe test for high concentrations of G. vaginalis
- OSOM BV Blue test (Sekisui Diagnostics, Framingham, MA), which detects vaginal fluid sialidase activity, have acceptable performance characteristics compared with Gram stain
- Nucleic Acid Amplification Tests (NAAT) are also available and “can be used as an alternative to clinical testing in settings where pH paper, KOH, and microscopy are not available”
- Do NOT use Pap tests
- Do NOT culture for G. vaginalis given normal vaginal flora is heterogenous

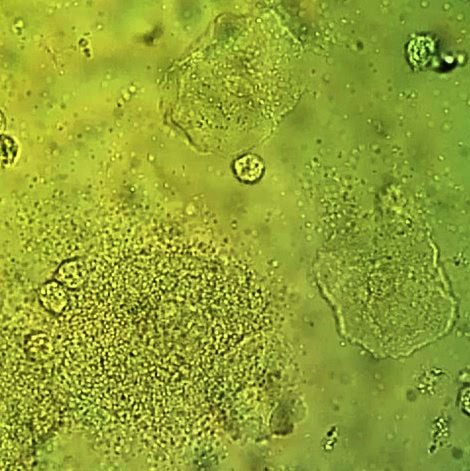
Vaginal wet mount with a NaCl preparation, showing a clue cell at bottom left, and two normal epithelial cells.
SYNOPSIS:
Bacterial Vaginosis (BV) is not caused by a single bacterium, but by high concentrations of facultative anaerobic bacteria (e.g., Prevotella sp. and Mobiluncus sp.), G. vaginalis, Ureaplasma, Mycoplasma, and numerous other anaerobes. BV is associated with multiple or new sex partners, lack of condom use and in particular lack of vaginal lactobacillus. Because BV is not an inflammatory condition, vulvar erythema and edema are not commonly seen, unlike candidiasis and trichomoniasis.
KEY POINTS:
Treatment is recommended for women with symptoms, including discharge, irritation and malodor and may reduce the risk for C. trachomatis, N. gonorrhoeae, T. vaginalis, HIV, and herpes simplex type 2.
Recommended CDC regimens include the following:
- Metronidazole* 500 mg orally twice a day for 7 days OR
- Metronidazole* gel 0.75%, one full applicator (5 g) intravaginally, once a day for 5 days OR
- Clindamycin** cream 2%, one full applicator (5 g) intravaginally at bedtime for 7 days
Alternative Regimens
- Tinidazole* 2 g orally once daily for 2 days OR
- Tinidazole* 1 g orally once daily for 5 days OR
- Clindamycin** 300 mg orally twice daily for 7 days OR
- Clindamycin** ovules 100 mg intravaginally once at bedtime for 3 days
- Secnidazole 2 g orally in a single dose
*Alcohol consumption should be avoided during treatment with oral nitroimidazoles. To reduce the possibility of a disulfiram-like reaction, abstinence from alcohol use should continue for 24 hours after completion of metronidazole and 72 hours after completion of tinidazole.
**Clindamycin ovules use an oleaginous base that might weaken latex or rubber products (e.g., condoms and vaginal contraceptive diaphragms). Use of such products within 72 hours following treatment with clindamycin ovules is not recommended.
- Test all women with BV for HIV and other sexually transmitted diseases (STDs)
- Follow-up visits are unnecessary if symptoms resolve
- Routine treatment of sex partners in not recommended
- Using a different recommended treatment regimen can be considered in women who have a recurrence
- Retreatment with the same recommended regimen is an acceptable approach for treating persistent or recurrent BV after the first occurrence
- Recurrent BV: At least 3 documented, separate episodes of BV in one year
- 0.75% metronidazole gel twice weekly for 4–6 months has been shown to reduce recurrences, although this benefit might not persist when suppressive therapy is discontinued
BV and Preterm Birth
- The USPSTF addresses BV screening during pregnancy and states the following
The USPSTF recommends against screening for bacterial vaginosis in pregnant persons not at increased risk for preterm delivery. (D recommendation)
The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for bacterial vaginosis in pregnant persons at increased risk for preterm delivery. (I statement)
Concurrent Sexual Partner Therapy
- Based on an RCT, ACOG recommends concurrent male sexual partner therapy
- For partners of patients with recurrent and symptomatic BV
- Male treatment incudes both oral and topical antimicrobial agents
- ACOG recommends shared decision making regarding concurrent sexual partner therapy for
- Same sex partners
- First occurrence of symptomatic bacterial vaginosis
- ACOG recommendations based on RCT (Vodstrcil et al. NEJM, 2025)
- Open-label, randomized controlled trial involving 164 heterosexual couples across five health centers in Australia
- Women received standard BV treatment
- Male partners were randomized to either receive oral metronidazole (400 mg) and 2% clindamycin cream applied to the penis, or no treatment
- Trial stopped at 12 weeks with only 150 couples due to inferiority of standard care
- Absolute risk difference: −2.6 recurrences per person-year (95% CI, −4.0 to −1.2; P<0.001)
- Limitations of the RCT include
- Population mostly derived from 1 sexual health service
- Results reflect outcomes in a higher-risk population that could impact generalizability
Note: BV partner treatment is not legally or clinically considered expedited partner therapy (EPT) under most state laws or CDC protocols (see ‘Primary Sources – Learn More’ Below for more information on EPT)
Learn More – Primary Sources:
Sexually Transmitted Infections Treatment Guidelines 2021
ACOG Practice Bulletin 215: Vaginitis in Nonpregnant Patients
USPSTF: Screening for Bacterial Vaginosis in Pregnant Persons to Prevent Preterm Delivery
Male-Partner Treatment to Prevent Recurrence of Bacterial Vaginosis (Vodstrcil et al. NEJM, 2025)
ACOG Clinical Update: Concurrent Sexual Partner Therapy to Prevent Bacterial Vaginosis Recurrence
STI Screening in Pregnancy: CDC Recommendations
CLINICAL ACTIONS:
Pregnant women are considered a ‘special population’ by the CDC. Due to the potential burden to pregnant women, offspring and partners, providers should ask all pregnant women and their partners about STIs, and ensure counseling, screening and treatment are available.
SPECIFIC STIs:
HIV
SYPHILIS
HEPATITIS B
HEPATITIS C
CHLAMYDIA
GONORRHEA
BACTERIAL VAGINOSIS
TRICHOMONAS
HSV-2
Recommended Screening Tests for ALL Pregnant Women
HIV
- ‘Opt-out screening’ – screen at first prenatal visit after notifying patient of the need to be screened, unless patient declines
- Screen in prepregnancy or as early as possible in pregnancy
- If patient declines, address concerns and discuss the following
- A previous negative HIV test does not mean patient is still negative
- Health benefit not only to patient but to fetus/offspring as treatment available to reduce perinatal transmission
- Retest in the 3rd trimester (before 36 weeks, if possible) if at high risk
- Illicit drug use
- STI during pregnancy
- Multiple sex partners during pregnancy
- Live in areas of high HIV incidence
- Receiving care in facilities with an HIV incidence in pregnant women ≥1/1,000 per year
- Partner has HIV
- Signs or symptoms of acute HIV infection
- Fever | Lymphadenopathy | Skin rash | Myalgias | Arthralgias | Headache | Oral Ulcers | Leukopenia | Thrombocytopenia | Elevated transaminase
- Rapid HIV testing should be performed on any woman in labor who has not been screened during pregnancy, unless she declines
- If rapid HIV test positive, antiretroviral prophylaxis should be administered prior to receiving confirmatory test results
- AAP recommends expedited HIV testing as soon as possible after birth for infants born to women with unknown HIV status
- NOTE: The USPSTF (June 2019) continues to recommend screening for HIV infection in all pregnant persons, including those who present in labor or at delivery whose HIV status is unknown. (A recommendation)
SYPHILIS
- Cases of congenital syphilis have increased 10 fold in the past decade
- Syphilis during pregnancy can lead to
- Stillbirth | Miscarriage | Infant death | Maternal and infant morbidity
- Serologic tests should be performed at first prenatal visit
- Screening for syphilis infection is a 2-step process | Antepartum screening can be performed by manual nontreponemal antibody testing (e.g., RPR) by using the traditional syphilis screening algorithm or by treponemal antibody testing (e.g., immunoassays)
- Traditional screening
- Initial “nontreponemal” antibody test (ie, Venereal Disease Research Laboratory test or rapid plasma reagin [RPR] test) to detect biomarkers released from damage caused by syphilis infection
- Followed by a confirmatory “treponemal” antibody detection test (ie, fluorescent treponemal antibody absorption [FTA-ABS] or T pallidum particle agglutination test [TP-PA])
- Reverse sequence screening algorithm
- Initial automated treponemal test (such as an enzyme-linked [EIA], chemiluminescence [CIA], or multiplex flow immunoassay [immunoblot])
- Followed by a nontreponemal test
- NOTE: If the test results of the reverse sequence algorithm are discordant, a second treponemal test (preferably using a different treponemal antibody) is performed
- Pregnant women with positive treponemal screening tests (e.g., EIA, CIA, or immunoblot) should have additional quantitative nontreponemal testing because titers are essential for monitoring treatment response
- If access to prenatal care is suboptimal, RPR test and treatment should be performed at time of pregnancy confirmation
- Serologic retesting in the 3rd trimester (28 weeks) and at delivery if the patient for patients at high risk including
- Sex with multiple partners | Sex in conjunction with drug use or transactional sex
- Late entry to prenatal care (i.e., first visit during the second trimester or later) or no prenatal care
- Methamphetamine or heroin use
- Incarceration of the woman or her partner
- Unstable housing or homelessness
- Test any woman who delivers a stillborn or in the case of infant death
- Untreated syphilis has a 40% infant death rate
- Do NOT discharge neonate if serologic status is unknown
- Newborn infection may not be immediately obvious
- Within a few weeks may develop
- Developmental delay
- Seizures
- Birth defects such as bone deformation, blindness and deafness
Note: In September 2018, the USPSTF reaffirmed previous guidance and “recommends early screening for syphilis infection in all pregnant women.” (Grade A – Offer or Provide this Service)
HEPATITIS B (HBV)
- Screen during each pregnancy, preferably in the first trimester, regardless of vaccination status or history of testing
- Use ‘triple panel’: Hepatitis B surface antigen (HBsAg), antibody to HBsAg, and total antibody to HBcAg (total anti-HBc)
- If patient underwent appropriately timed triple panel screening and has not had any new HBV exposures since triple panel screening, only HBsAg screening is required
- At time of admission for delivery, retest if patient
- Is at high risk – more than one sex partner in previous 6 months, evaluation or treatment for STI, injection-drug use, HBsAG-positive sex partner
- Was not screened prenatally
- Has clinical hepatitis
- Always do HBsAg testing prior to giving the HBV vaccine to avoid misinterpretation
- Report HBsAg positive women to local or state health departments to ensure they are entered into a case management program to arrange access to appropriate vaccinations for contacts and prophylaxis for infants
- If HBsAg positive, test for hepatitis B virus deoxyribonucleic acid (HBV DNA) to guide the use of antiviral medication to prevent perinatal transmission
- If HBV DNA >200,000 IU/mL (7.6 log10 IU/mL): The American Association for the Study of Liver Diseases suggests antiviral therapy during pregnancy to further reduce perinatal HBV transmission
HEPATITIS C (HCV)
- The CDC has updated HepC guidelines (2020)
- Hepatitis C screening at least once in a lifetime for all adults aged ≥18 years, except in settings where the prevalence of HCV infection (HCV RNA-positivity) is <0.1%
- Hepatitis C screening for all pregnant women during each pregnancy, except in settings where the prevalence of HCV infection (HCV RNA-positivity) is <0.1%
- USPSTF also calls for universal screening for HCV infection, including pregnancy
Recommended Screening Tests for Pregnant Women at Risk
CHLAMYDIA
- Test all pregnant women who are <25 years old for Chlamydia trachomatis at the first prenatal visit
- Test all older women if at high risk:
- More than one sex partner
- A sex partner with concurrent partners or has an STI
- Retest in the 3rd trimester to prevent maternal postnatal complications and chlamydia infection in the neonate
- Test of cure by NAAT 3 to 4 weeks after treatment and retest within 3 months
GONORRHEA
- Test all pregnant women who are <25 years old for N. gonorrhoeae at the first prenatal visit
- Test all older women if at high risk:
- More than one sex partner
- A sex partner with concurrent partners or has an STI
- Inconsistent condom use in non-monogamous relationships
- Previous or co-existing sexually transmitted infections
- Exchanging sex for money or drugs
- Consider consulting local public health authorities for further guidance on identifying those at high risk related to geographic location
- Treat all positive patients immediately and retest in 3 months
- Retest in the 3rd trimester to prevent maternal postnatal complications and chlamydia infection in the neonate
Screen Only if Symptomatic
Bacterial Vaginosis (BV)
- Evidence does not support routine screening
- Evaluate and screen symptomatic women
- The USPSTF addresses BV screening during pregnancy and states the following
The USPSTF addresses BV screening during pregnancy and states the following
The USPSTF recommends against screening for bacterial vaginosis in pregnant persons not at increased risk for preterm delivery. (D recommendation)
The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for bacterial vaginosis in pregnant persons at increased risk for preterm delivery. (I statement)
Trichomonas
- Evidence does not support routine screening
- Evaluate and screen symptomatic women
HSV-2
- Evidence does not support routine screening
- In the absence of lesions during the 3rd trimester, routine cultures for HSV are not indicated for women in the 3rd trimester who have a history of recurrent genital herpes
- Type-specific serologic tests may help identify pregnant women at risk for HSV and to help guide counseling regarding the risk of acquiring herpes during pregnancy
SYNOPSIS:
Recommendations for STI testing can vary based on certain considerations, including state laws. The CDC recommendations are considered broader, such that more women will potentially be screened, but are consistent with other CDC guidance with the intention of preventing adverse outcomes for pregnant women, partners and fetuses.
KEY POINTS:
- All pregnant women and their partners should be asked about STIs and counseled regarding personal risks as well as pregnancy and outcomes
- Pap Smears should be performed in pregnancy at the same frequency as nonpregnant women
- Management of abnormal Pap tests differ in pregnancy
Screening at Delivery
SYPHILIS
- Select groups of pregnant women, including women who are at high risk for syphilis or live in areas of high syphilis morbidity
- Pregnant women with no previously established status
- Pregnant women who deliver a stillborn infant
HIV
- Pregnant women not screened during pregnancy
HBV
- Women admitted for delivery at a health care facility without documentation of HBsAg test results should have blood drawn and tested as soon as possible after admission
- Women at high risk
- Having had more than one sex partner during the previous 6 months, an HBsAg-positive sex partner, evaluation or treatment for a sexually transmitted disease, or recent or current injection-drug use
- Women with signs or symptoms of hepatitis
Note: CDC recommends universal hepatitis B vaccination within 24 hours of birth for medically stable infants >2000 grams
- Permissive language that allowed the vaccine to be delayed until after hospital discharge has been removed
- Administer hepatitis B vaccination and hepatitis immune globulin regardless of birth weight within 12 hours of birth for infants born to hepatitis b-infected mothers
CHLAMYDIA
- Pregnant women less than 25 years of age
- Continued high risk
- New or multiple sex partners, sex partner with concurrent partners, sex partners who have a sexually transmitted disease
GONORRHEA
- Continued high risk
- Past or current injection-drug use, having had a blood transfusion before July 1992, receipt of an unregulated tattoo, having been on long-term hemodialysis, intranasal drug use, and other percutaneous exposures
Learn More – Primary Sources:
CDC: Sexually Transmitted Infections Treatment Guidelines 2021
Current Perspectives on Prevention of Mother-to-Child Transmission of Syphilis
ACOG Committee Opinion 752: Prenatal and Perinatal Human Immunodeficiency Virus Testing: Expanded Recommendations
CDC: A Guide to Taking a Sexual History
CDC: Prevention of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices
ACOG Clinical Practice Guideline 6: Viral Hepatitis in Pregnancy
CDC Recommendations for Hepatitis C Screening Among Adults — United States, 2020
Screening for Syphilis Infection in Pregnant Women: US Preventive Services Task Force Reaffirmation Recommendation Statement
Screening for HIV Infection: US Preventive Services Task Force Recommendation Statement
Screening for Hepatitis B Virus Infection in Pregnant Women: US Preventive Services Task Force Reaffirmation Recommendation Statement
USPSTF: Screening for Bacterial Vaginosis in Pregnant Persons to Prevent Preterm Delivery
Screening and Testing for Hepatitis B Virus Infection: CDC Recommendations — United States, 2023
Vital Signs: Missed Opportunities for Preventing Congenital Syphilis — United States, 2022
Screening for Sexually Transmitted Infections – Who, When and How Often?
SYNOPSIS:
There are an estimated 2.8 million new chlamydia infections each year in the US and 1.5 million new cases of gonorrhea diagnosed. The highest rates of both gonorrhea and chlamydia are reported in women aged 15 to 24. Symptoms are vague and sequelae can include pelvic inflammatory disease, ectopic pregnancy and infertility. A full comprehensive sexual history may identify other risk factors to prompt more comprehensive screening for sexually transmitted infections
CLINICAL ACTIONS:
Sexually transmitted infections (STIs) are common with potential for serious long term outcomes, and remain a serious public health concern. Here, we outline the recommendations for screening for STIs by population:
General Population
Gonorrhea and Chlamydia
- Annual screening for gonorrhea and chlamydia is recommended for all sexually active women <25 years | evidence is insufficient for routine testing of gonorrhea and chlamydia in heterosexual men, consider screening young men in high prevalence clinical settings e.g. adolescent clinics, correctional facilities, STI/sexual health clinic
- Re-testing is recommended 3 months after treatment due to high re-infection rates
- Screening is recommended for adults >25 years old at increased risk for infection (new partner, multiple partners, or a partner who has an STI)
- Consider testing for rectal chlamydia and pharyngeal gonorrhea based on sexual history practices
- Annual testing is recommended for men who have sex with men (MSM) at sites of contact (urethra, rectum)and every 3-6 months if at higher risk e.g. MSM on pre-exposure prophylaxis (PrEP), HIV infection, or if they or their sex partners have multiple partners
- Transgender and Gender Diverse Persons screening adapted based on anatomy
The USPSTF 2021 Update: Chlamydia and Gonorrhea Screening
…recommends screening for chlamydia in all sexually active women 24 years or younger and in women 25 years or older who are at increased risk for infection. (B recommendation)
…recommends screening for gonorrhea in all sexually active women 24 years or younger and in women 25 years or older who are at increased risk for infection. (B recommendation)
The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for chlamydia and gonorrhea in men
Syphilis
- Screening for syphilis is based on risk profile, with higher risk including history of incarceration, transactional sex work, geography, or male younger than 29 years old
- Annual screening for sexually active MSM | 3 to 6 months if at increased risk
- Annual screening for syphilis is recommended in transgender and gender diverse persons
HSV
- Consider type-specific HSV serologic testing in patients presenting for an STI evaluation (especially if multiple partners)
Note: USPSTF “recommends against routine serologic screening for genital HSV infection in asymptomatic adolescents and adults, including those who are pregnant”
Trichomonas
- Consider screening for trichomonas in high-prevalence settings or patients at higher risk for infection (multiple sex partners, transactional sex, drug misuse, or a history of STI or incarceration)
Hepatitis B
- Screen all adults aged ≥18 years at least once during a lifetime (CDC recommendation)
- Use triple Panel: 3 main serologic markers used to determine HBV infection status
- Hepatitis B surface antigen (HBsAg) | Antibody to hepatitis B surface antigen (anti-HBs) | Antibody to hepatitis B core antigen (anti-HBc)
- Test individuals with a history of risk for HBV infection, regardless of age, if they might have been susceptible during the period of risk
- Susceptible persons include those who have never been infected with HBV (i.e., total anti-HBc negative) and either did not complete a HepB vaccine series per ACIP recommendations or who are known vaccine nonresponders
- Periodically test susceptible persons, regardless of age, who have ongoing risk | Offer testing if the risk for exposure occurred after previous HBV serologic testing and while the person was susceptible
- CDC expands risk-based testing recommendations to the following populations
- Activities, exposures, or conditions associated with increased risk for HBV infection
- Persons incarcerated or formerly incarcerated in a jail, prison, or other detention setting
- Persons with a history of STIs or multiple sex partners
- Persons with a history of hepatitis C virus infection
- Offer testing to anyone who requests HBV testing
Hepatitis C
- Screening for hepatitis C infection (HCV) should include
- All adults 18 and older at least once in their lifetime
- Pregnant women, during each pregnancy
- CDC recommends at least one-time testing for
- People who currently or with history of injecting drugs
- People who have HIV
- People with abnormal liver tests, liver disease, or who are on hemodialysis
- People who received blood or organ donations before July 1992
- People who received clotting factor concentrate before 1987
- Health care, emergency medical, and public safety personnel after needle sticks, sharps, or mucosal exposures to HCV-positive blood
- Infants and children born to people with known HCV infection
- CDC recommends periodic testing for
- People with ongoing risk factors, including people who currently inject drugs and share needles, syringes, or other drug equipment
- People with certain medical conditions, including those who have ever received maintenance hemodialysis
- Any person who requests hepatitis C testing
HIV
- Screening for HIV should be performed in all individuals aged 15 to 65 | Younger adolescents and older adults who are at increased risk of infection should also be screened
- Annual HIV screening is recommended for MSM with more than one sexual partner, with consideration for more frequent 3-6 month intervals for testing
- The USPSTF recommends screening for HIV in all pregnant persons, including those who present in labor or at delivery whose HIV status is unknown
- People who are at increased risk for HIV should be screened at least annually
- People who inject drugs and their sex partners
- People who exchange sex for money or drugs
- Sex partners of people with HIV
- Sexually active gay, bisexual, and other men who have sex with men (more frequent testing may be beneficial [e.g., every 3–6 months])
- Heterosexuals who themselves or whose sex partners have had ≥1 sex partner since their most recent HIV test
- People receiving treatment for hepatitis, tuberculosis, or STIs
Persons Living With HIV
- At first HIV evaluation and annually afterwards, screen for
- Gonorrhea
- Chlamydia
- Syphilis
- Hepatitis B surface antigen and Hepatitis B immunity
- Hepatitis C screening for all persons with HIV and subsequent annual testing for MSM
- Specifically for women with HIV
- Screen for trichomonas for women at first evaluation and annually afterwards
- Women should be screened within 1 year of sexual activity with testing repeat 65 months later | 3 normal and consecutive pap tests, screening can be spaced out to every 3 years
- For pregnant women: repeat testing during the third trimester in women with risk factors and in women living or receiving care in high-incidence settings who had a negative test result earlier in pregnancy | CDC notes that repeat testing in the third trimester may be considered for all women with a negative test result early in pregnancy
KEY POINTS:
- Screen sexually active women ≥25 for gonorrhea and chlamydia if at increased risk
- More comprehensive screening for STIs include evaluation for trichomonas, syphilis, HIV, Hepatitis B and Hepatitis C
- CDC has updated guidelines to recommend universal Hepatitis C and Hepatitis B screening in all adults
Learn More – Primary Sources:
CDC: Sexually Transmitted Infections Treatment Guidelines 2021
CDC: A Guide to Taking a Sexual History
CDC: Screening and Testing for Hepatitis B Virus Infection 2023
CDC: Clinical Screening and Diagnosis for Hepatitis C
USPSTF: Screening for Chlamydia and Gonorrhea
USPSTF: Serologic Screening for Genital Herpes Infection
USPSTF: Recommendation: Human Immunodeficiency Virus (HIV) Infection Screening