Bioidentical hormones are hormones that are created synthetically in a laboratory and are designed to have a chemical structure that is identical tohormones in the human body. There is significant confusion both in the lay and professional community regarding bioidentical hormones, what they are, what they are not and understanding their safety profile.
Bioidentical hormones
Are not necessarily natural or botanical
May or may not be created in a compounding pharmacy
May also be created in an FDA approved laboratory
Are not necessarily “healthy” nor “safe”
Bioidentical hormones which are FDA-approved and regulated, may be safer than ones created in a compounding pharmacy as those may be subject to human error and are not subject to the rigorous standards and regulations of the FDA
Many prescription hormones are bioidentical
Drug companies often develop non-bioidentical hormones because they can then be patented, while bioidentical ones cannot
When hormones are bioidentical the only way the drug company can patent them is by creating a new or different “delivery system”
For example, drug delivery by a “patch” or use of a different compound to deliver the drug
‘Regulated body-identical hormone therapy (rBHT)’ is a term that is used by some to help differentiate between regulated from unregulated forms of bioidentical hormones
ACOG states
Clinicians should counsel patients that FDA-approved menopausal hormone therapies are recommended for the management of menopausal symptoms over compounded bioidentical menopausal hormone therapy
HPV Vaccine Recommendations Including Guidance for Ages 27 to 45
SUMMARY:
The most recent evidence-based HPV vaccine recommendations address when to administer the vaccine and dosing. One area that has elicited more recent guidance focuses on whether to offer the HPV vaccine to individuals over the age of 26.
The FDA (October 2018) extended approval of HPV vaccine to individuals age 27 to 45 years
ACIP (June 2019) voted to
Expand routine and catch-up HPV vaccination in males through 26 years of age who are inadequately vaccinated
Offer HPV vaccine to individuals age 27 to 45 years who have not been adequately vaccinated based on shared clinical decision making
ACIP published their final recommendations (August 2019) in the CDC’s Morbidity and Mortality Weekly Report
Children and adults aged 9 through 26 years: HPV vaccination is routinely recommended at age 11 or 12 years; vaccination can be given starting at age 9 years. Catch-up HPV vaccination is recommended for all persons through age 26 years who are not adequately vaccinated.
Adults aged >26 years: Catch-up HPV vaccination is not recommended for all adults aged >26 years. Instead, shared clinical decision-making regarding HPV vaccination is recommended for some adults aged 27 through 45 years who are not adequately vaccinated. HPV vaccines are not licensed for use in adults aged >45 years.
These recommendations for children and adults aged 9 through 26 years and for adults aged >26 years apply to all persons, regardless of behavioral or medical risk factors for HPV infection or disease.
For persons who are pregnant, HPV vaccination should be delayed until after pregnancy; however, pregnancy testing is not needed before vaccination.
Persons who are breastfeeding or lactating can receive HPV vaccine. Recommendations regarding HPV vaccination during pregnancy or lactation have not changed.
ACIP suggests considering the following points for shared-decision making with adults who are 27 to 45 years of age
HPV is very common, usually transient and asymptomatic
Although typically acquired in young adulthood, some adults are at risk for acquiring new HPV infection
A new sex partner is a risk factor, while those in long-term, mutually monogamous partnerships are not likely to acquire a new HPV infection
HPV types: Sexually active adults will likely have been exposed to some HPV types, but not all HPV types are vaccine targets
There is no antibody test to determine immunity
HPV vaccine has high efficacy in young persons not yet exposed to vaccine-type HPV
Lower vaccine effectiveness may be expected in those with HPV risk factors
Multiple lifetime sex partners | Previous infection with vaccine-type HPV | immunocompromising conditions
HPV vaccines are prophylactic only and can’t prevent infection progression, improve time to clearance or treat HPV-related disease
In summary, the CDC states
For adults aged 27 years and older, clinicians can consider discussing HPV vaccination with people who are most likely to benefit. HPV vaccination does not need to be discussed with most adults over age 26 years
CDC Dosing Schedule
<15 years: 2 doses spaced 6 to 12 months apart
≥15 years: 3-dose schedule
Initial dose
Second dose at 1 to 2 months after initial
Third dose at 6 months after initial
Updated ACOG HPV vaccine recommendations
Routine HPV vaccination is recommended for females and males
Target age is 11 to 12 years but can be given through age 26
Can be given from age of 9
Do not test for HPV DNA prior to vaccination
Vaccinate even if patient was tested and is HPV DNA positive
If not vaccinated between 11 to 12 years
Vaccinate between 13 to 26 years (catch up period)
Women 27 to 45 years and not previously unvaccinated
Use shared clinical decision making
ACOG “does not recommend that an individual who received the quadrivalent HPV vaccine be revaccinated with 9-valent HPV vaccine, including those aged 27–45 years who previously completed some, but not all, of the vaccine series when they were younger”
Pregnancy
HPV vaccine is not recommended during pregnancy
Pregnancy testing prior to HPV vaccination not recommended
If vaccination schedule is interrupted by pregnancy, resume postpartum with the next dose
HPV vaccine can and should be given to breastfeeding women ≤26 who have not been vaccinated
Counsel to expect mild local discomfort and that this is not a cause for concern
Watch adolescents for at least 15 minutes following vaccination due to risk of fainting in this population
AAP
The AAP has also endorsed the CDC HPV recommendations
The HPV vaccine should be normalized as a standard of care
Recommendation should be clear and unambiguous
AAP provides multiple strategies (see ‘Learn More – Primary Sources’ below) to engaging with patients including focusing on cancer prevention benefits for all children
ACS
The ACS endorses ACIPCDC guidance regarding HPV guidance except for the approach to take with individuals who are 27 to 45 years and not adequately vaccinated
The ACS does not endorse the 2019 Advisory Committee on Immunization Practices recommendation for shared clinical decision making for some adults aged 27 through 45 years who are not adequately vaccinated because of the low effectiveness and low cancer prevention potential of vaccination in this age group, the burden of decision making on patients and clinicians, and the lack of sufficient guidance on the selection of individuals who might benefit
Adjuvant HPV Vaccine to Prevent CIN Recurrence
ACOG recommends considering adjuvant HPV vaccine for unvaccinated individuals 27 to 45 years who are undergoing treatment for CIN 2+
Masses of the ovary, fallopian tube or other pelvic organs may be incidental findings on examination or may present with symptoms of pain. The diagnostic evaluation determines need for and type of surgical or medical intervention.
CLINICAL ACTIONS:
Obtain a medical, gynecologic and family history and review of systems
Evaluate vital signs and general appearance
Exam should include assessment of cervical, supraclavicular, axillary and groin nodes as well as breast, abdominal and pelvic examination
Clinical findings suggestive of malignancy include
Irregular contour
Firm
Fixed
Nodular
Bilaterality
Ascites
Imaging
Ultrasound
Obtain transvaginal ultrasound to assess mass for findings suggestive of malignancy including
Transvaginal sono is not possible (e.g., young, virginal or prepubertal)
Ultrasound algorithms to predict malignancy (see ‘Related ObG Topics’ below)
IOTA group: Simple Rules
Other algorithms also available
Other Imaging Modalities
CT, MRI and PET are not recommended as ‘first line’ imaging modalities
MRI can help differentiate origin of mass when unclear
CT scan can be helpful to evaluate abdomen when cancer is suspected
MRI and CT may be used to as an adjunct in the work up of suspected cystic teratomas (differentiates lipid densities)
Serum Markers
Biomarkers can be used in the evaluation of a pelvic mass but are not currently recommended for use in population based screening for ovarian cancer
CA 125
Overall wide range of sensitivity and specificity, especially in premenopausal women
PPV: 5% to 91%,
NPV: 67% to 90%
Postmenopausal
PPV of CA 125 is higher in postmenopausal women
Elevated CA 125 and pelvic mass in postmenopausal woman warrants referral to Gyn Oncologist
Premenopausal
Less valuable but extreme values warrant caution and raised suspicion
No evidence-based threshold currently exists for premenopause
Other causes: Fibroids | Endometriosis | PID | Ascites (not necessarily related to ovarian cancer) | Medical disorders with inflammatory component
Biomarker Panels
Two FDA approved serum tumor marker panel tests, for use in women >18 years with an already identified adnexal mass that requires surgery
Multivariate index assay
Combination of CA 125 II | Transferrin | Transthyretin (prealbumin) | Apolipoprotein A-1 | ß 2-microgloblin
Translates into a malignancy risk score of 0-10 using proprietary algorithm
“…higher sensitivity and negative predictive value for ovarian malignancy when compared with clinical impression and CA 125 alone”
Sensitivity increases with additional clinical assessment and inclusion of ultrasound findings
Risk of Ovarian Malignancy Algorithm
Combination of CA 125 | Human epididymis protein 4 | Menopausal status
Algorithm based on variable cut-off values related to menopausal status
Epididymis protein 4 is more sensitive and specific than CA 125
ACOG states
Serum biomarker panels may be used as an alternative to CA 125 level alone in determining the need for referral to or consultation with a gynecologic oncologist when an adnexal mass requires surgery
Other Markers
If suspicious for less common tumors (e.g. germ cell), consider
ß-hCG | L-LDH | AFP
Granulosa cell tumors (solid mass and postmenopausal bleeding)
Inhibin | Estrogen
SYNOPSIS:
Evaluation of the patient with an adnexal mass is intended to exclude malignancy, identify patients in need of emergent surgery and allow appropriate scheduling for those who need nonemergent surgery. Patients with tubo-ovarian abscesses may respond to medical management or interventional radiologic drainage. Those with small cysts can often be followed with ultrasound in anticipation of spontaneous resolution. Metastatic cancers, especially from breast, colon or stomach may present as adnexal masses. Those with findings suggestive of malignancy should have consultation with or referral to a gynecologic oncologist.
KEY POINTS:
Age and a strong family history of breast or ovarian cancer remain important risk factors for ovarian malignancy
Transvaginal ultrasonography is the recommended imaging for pelvic masses
Findings of concern include: cyst size greater than 10 cm, papillary or solid components, irregular shape, ascites, high color Doppler flow
Benign masses will generally show the following on ultrasound
Thin, smooth walls, no solid components or septation, no internal blood flow on color Doppler
Simple cysts over 10 cm are generally considered an indication for surgery but may resolve over time
Serum marker testing in combination with other tests can be used to evaluate likelihood of malignancy
Note: The ESGO/ISUOG/IOTA/ESGE Consensus Statement (see ‘Learn More – Primary Sources’ below) provides excellent summary tables on clinical and ultrasound features of adnexal masses
When to Observe
Ultrasound suggests benign disease
Ultrasound findings unclear but there is a good reason to try and avoid surgery
Normal CA 125 level and no suspicious ultrasound findings
<10 cm simple cysts, even in postmenopause can be observed with repeat imaging
The ideal interval and duration for ultrasound follow-up has yet to be defined. However, in one study, masses that were monitored and eventually diagnosed as malignancies all demonstrated growth by 7 months . Some experts recommend limiting observation of stable masses without solid components to 1 year, and stable masses with solid components to 2 years.
When to Refer to Gyn Oncology
Postmenopausal
Elevated CA 125 | Suspicious ultrasound or clinical findings
Premenopausal
Very elevated CA 125 level | Suspicious ultrasound or clinical findings
Premenopausal or postmenopausal
Elevated score on a formal biomarker risk assessment test or ultrasound-based scoring systems from the IOTA group
ACOG & SMFM Guidance on the Use of IUDs and Contraceptive Implants
SUMMARY:
IUDs and etonogestrel single-rod contraceptive implants are categorized as Long-Acting Reversible Contraception (LARC). ACOG and other professional and public health entities are calling for reduced barriers and improved access to LARC. The latest ACOG practice bulletin reviews various LARC options, including clinical considerations such as use in the postpartum period and management in the setting of pelvic infections. ACOG has also released an updated ‘Quick Coding Guide’ for LARC that can be found in ‘Learn More – Primary Sources’ section.
Subdermal implant with a core containing 68 mg of etonogestrel
FDA approved for 3 years
Clinical Considerations
Nulliparous and Adolescents
LARCs should be offered routinely as safe and effective contraceptive options for nulliparous women and adolescents
Use of LARCs in adolescents supported by the AAP
IUD
MEC category 2 (advantages outweigh risks)
Risk of infection is low
No evidence of association with infertility or tubal occlusion
High satisfaction rate based on continuation rates
Expulsion rates may be higher in adolescents vs older women and multiparous vs nulliparous
Like the general population, nulliparous women and adolescents prefer LNG-IUD
Implant
MEC category 1 (no restrictions)
Continuation rates higher in adolescents compared to OCPs
SMFM Guidance on Women at High Risk for Medical Complications (2019)
Use of LARC is encouraged for women at highest risk for adverse health events as a result of a future pregnancy (GRADE 1B)
SMFM recommends discussion take place in the prenatal period regarding availability of immediate postpartum LARC and MEC guidelines should be used to determine best method for particular medical conditions (GRADE 1C)
Counseling should include discussion around expulsion rates but appear to be outweighed by benefit of higher continuation rates (GRADE 1C)
Providers who intend to utilize immediate postpartum LARC should obtain appropriate training (Best Practice)
SMFM recommends that for women who are eligible and desire LARC, following a high-risk pregnancy, immediate postpartum LARC should be used vs delayed placement due to overall superior efficacy and cost-effectiveness (GRADE 1B)
Encourage breastfeeding following immediate postpartum LARC based on current evidence (GRADE 1B)
SMFM suggests that if a women wishes and is eligible for LARC, but immediate postpartum is not feasible, consider early postpartum placement (GRADE 2C)
Contraceptive counseling should be (Best Practice)
Patient-centered
Within a shared decision-making framework
Timing of Insertion
Interval insertion
Insertion may be performed at any time during menstrual cycle if patient is not pregnant
No benefit to inserting during menses
Postabortion LARC Insertion
Routinely offer immediate insertion following first trimester and second trimester abortion (induced or spontaneous)
Postpartum LARC Insertion
Offer immediate LARC insertion (IUD and implant) prior to hospital discharge
Higher IUD expulsion rates (10-27%), but cost-benefit supports immediate insertion
Considered ACOG ‘best practice’
Waiting 4-6 weeks may result in barrier to access
Contraindications to IUD placement include chorioamnionitis, endometritis, or puerperal sepsis or ongoing postpartum hemorrhage
Effect on Breastfeeding
Copper IUD: No hormonal concerns
LNG-IUD and implant: Studies do not demonstrate a deleterious effect on breast feeding including milk volume/composition, newborn weight or exclusive breastfeeding rates
ACOG recommends shared decision making regarding concerns
Patients should be counseled regarding
Theoretical risk of reduced duration of breastfeeding
Lack of data supporting a negative association
Infection Risk and IUD
Asymptomatic women who are at low risk of STDs and have undergone routine screening
No additional screening required at the time of IUD insertion
Women who have not been screened for STDs or at increased risk for STDs
Requires CDC-recommended STD screening at the time of a single visit for IUD insertion
Do not delay IUD placement while waiting on results
Treat a positive test without removing the IUD
Purulent cervicitis is a contraindication to IUD placement
If known chlamydia or gonorrhea infection, delay IUD insertion following infection treatment until
Antibiotic course is complete
Symptoms resolved
Pelvic/cervical exam normal
Repeat testing at 3 months for gonorrhea or chlamydia to rule out reinfection
Routine antibiotic prophylaxis is not recommended prior to IUD insertion
Actinomyces on cytology is an incidental finding
No treatment or IUD removal required if patient is asymptomatic
Pregnancy with IUD in situ
Determine location of pregnancy to rule out ectopic pregnancy
Remove IUD if strings visible as benefits outweigh risks
If patient opts to retain IUD, counsel regarding risks (which are not totally eliminated by IUD removal)
Providers keep medical charts for the purpose of providing good care, retaining accurate notes and, when necessary, sharing valuable information with colleagues. Even after a patient has left care, it is not unusual to receive a request for records. Patients may move or there may be important medical history that can help diagnose another family member at some point in the future (e.g., heritable cancer syndromes). Additionally, a well-documented medical record is always the best defense against a medical malpractice lawsuit. As courtroom adage goes, if it isn’t documented, it didn’t happen.
Notes made in the medical record at or near the time of treatment are regarded as highly reliable evidence. Without medical records, healthcare providers might not be able to show what care was provided and whether it met the standard of care. Simply stating the level of care and treatment rendered without providing documentation will often not succeed in a court of law, thus leaving the provider liable for the patient’s alleged injuries.
State and Federal Laws
State and federal laws regarding mandatory record retention requirements for hospitals or similar facilities differ from the laws for physician practices. The retention period for a minor’s records also varies. This variation exists to allow minors to bring suit for medical malpractice after they reach the age of majority for injuries that occurred when they were under age.
Generally, the Medicare Conditions of Participation (COP) require hospitals to retain records for five years (six years for critical access hospitals). HIPAA privacy regulations require records to be retained for six years from when the record was created to adhere to the federal statute of limitations for civil penalties for HIPAA violations. See record retention requirements from the healthit.gov site in ‘Learn More – Primary Sources’ below.
Medical Board and Medical Association Policies and Recommendations
When a direct state or federal law does not specify the retention period for physicians, medical boards may be able to provide policies or recommendations on how long a physician should keep records. For example, the Colorado State Board of Medical Examiners Policy 40-07 requires retaining all patient records for a minimum of 7 years after the last date of treatment, or 7 years after the patient reaches age 18 – whichever occurs later.
Storage and Safety Considerations
With the near mandatory use of electronic medical records, the storage of paper records will slowly be eliminated. However, attendant with the use of EMR comes the ever increasing need to prevent loss of data, or worse, hacking and cyber attacks on the electronic data across all industries. Antiquated infrastructure and uncorrected network vulnerabilities are frequent causes of successful attacks.
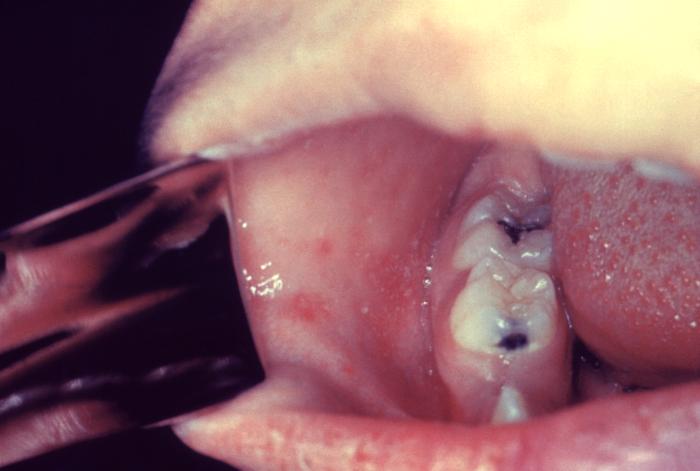
Otitis Media: 1/10 children and may result in permanent hearing loss
Severe complications in children requiring hospitalization
Acute encephalitis: 1/1,000 children, resulting in permanent brain damage
Respiratory and neurologic: 1/1,000 children will die from these complications
Subacute sclerosing panencephalitis (SSPE): Rare, fatal degenerative disease of CNS, resulting in deterioration and seizures 7 to 10 years after measles infection
Diagnosis and Testing
Clinical suspicion
Signs and symptoms detailed above
Special concern for those traveling internationally or exposed to someone with a febrile rash illness
Laboratory confirmation
Essential for all sporadic measles cases and all outbreaks
A capture IgM EIA (non-quantitative) that incorporates a recombinant measles nucleocapsid protein as the antigen is used to detect measles IgM
A commercial, indirect EIA (non-quantitative) assay is used to detect IgG
Viral detection methods: Includes real time RT-PCR to detect measles viral RNA | Available at many state public health laboratories and though the APHL/CDC Vaccine Preventable Disease Reference Centers (see ‘Learn More – Primary Sources’ below)
Detection of measles-specific IgM antibody in serum and measles RNA by RT-PCR in a respiratory specimen are the most common methods for confirming measles infection
Obtain both a serum sample and a throat swab (or nasopharyngeal swab) from patients suspected to have measles at first contact
Urine samples may also contain virus: If possible collect both respiratory and urine samples
Public Health: Molecular analysis (genotyping) can map transmission pathways of measles viruses
Evidence of Immunity
Note: Do not accept verbal reports of immunity
Acceptable presumptive evidence of immunity against measles includes ≥1 of the following
Written documentation of one or more doses of a measles-containing vaccine administered on or after the first birthday for preschool-age children and adults not considered high risk
Written documentation of two doses of measles-containing vaccine for school-age children and adults at high risk, including students at post-high school secondary educational institutions, healthcare personnel, and international travelers
Laboratory evidence of immunity *
Laboratory confirmation of measles
Birth before 1957
*Note: CDC addresses laboratory evidence of immunity and states the following
*People who have negative or equivocal results for measles IgG should be vaccinated or revaccinated. In some cases it is not possible to vaccinate a patient, and you may need to test them with a second line diagnostic assay to determine whether they are immune to measles. Because the sensitivity and specificity of commercial measles IgG assays vary, state public health departments can provide information on appropriate second line assays.
NOTE FOR HEALTHCARE PERSONNEL (HCP): CDC has interim guidance that states
Consider vaccinating HCP born before 1957 who do not have other evidence of immunity to measles
During a measles outbreak, 2 doses of measles virus-containing vaccine are recommended for all HCP, regardless of year of birth
See more HCP interim guidance using the CDC link below in ‘Learn More – Primary Sources’
Measles Vaccine Recommendations (CDC)
Children – MMR vaccine
First dose: 12 through 15 months of age
Second dose: 4 through 6 years of age no earlier than 28 days following the first dose
Students at post-high school educational institutions without evidence of measles immunity
2 doses of MMR vaccine
Second dose administered no earlier than 28 days after the first dose
Adults born ≥1957 who do not have evidence of measles immunity
Should get at least one dose of MMR vaccine
International travelers ≥6 months of age
Infants 6 through 11 months: one dose of MMR vaccine
One dose at 12 through 15 months of age and another dose at 4 through 6 years of age or at least 28 days later
Infants who get one dose of MMR vaccine before their first birthday should get two more doses according to the routinely recommended schedule
Children ≥12 months: Documentation of two doses of MMR vaccine (the first dose of MMR vaccine should be administered at age 12 months or older; the second dose no earlier than 28 days after the first dose)
Teenagers and adults born ≥1957 (no immunity): Documentation of two doses of MMR vaccine, with the second dose administered no earlier than 28 days after the first dose
Post-exposure Prophylaxis
Cannot Readily Show Evidence of Immunity Following Exposure to Measles
Offer post-exposure prophylaxis (PEP) or be excluded from the setting (school, hospital, childcare)
Unvaccinated individuals who receive their first dose of MMR vaccine within 72 hours after exposure may return to childcare, school, or work except healthcare workers
PEP: Administer MMR vaccine within 72 hours of initial measles exposure or immunoglobulin (IG) within six days of exposure
Monitor for signs and symptoms consistent with measles for at least one incubation period following PEP
Note: “Do not administer MMR vaccine and IG simultaneously, as this practice invalidates the vaccine”
MMR vaccine for PEP
Should still offer MMR vaccine even if beyond 72 hours to protect from future exposures
Outbreak control measure for infants <12 months of age: Measles vaccination of infants as young as 6 months of age may be used (revaccinate when they are 12 through 15 months old and again when they are 4 through 6 years of age)
Immunoglobulin (IG) for PEP
IG dosing
IGIM dose: 0.5 mL/kg of body weight (maximum dose = 15 mL)
IGIV dose: 400 mg/kg
IG used for high risk populations
Infants younger <12 months
Intramuscular IG (IGIM) for all
However, if 6 through 11 months, MMR vaccine can be given in place of IG, if administered within 72 hours of exposure
Pregnant women without evidence of measles immunity
Intravenous IG (IGIV)
Severely compromised immune systems
Administer IGIV regardless of immunologic or vaccination status
Note: People cannot return to healthcare settings following receipt of IG | For other settings, such as childcare, school, or work “factors such as immune status, intense or prolonged contact, and presence of populations at risk, should be taken into consideration before allowing people to return”
PEP for healthcare personnel
MMR vaccine should be given within 72 hours or IG should be given within 6 days
“Exclude healthcare personnel without evidence of immunity from duty from day 5 after first exposure to day 21 after last exposure, regardless of post-exposure vaccine”
Isolation
Isolate for four days after they develop a rash
Use airborne precautions in healthcare settings
All healthcare staff entering the room should use respiratory protection consistent with airborne infection control precautions (use of an N95 respirator or a respirator with similar effectiveness in preventing airborne transmission)
Use single-patient airborne infection isolation room (AIIR) for patient with measles
People without evidence of immunity who have been exempted from measles vaccination for medical, religious and now PEP within appropriate timeframe
Exclude from affected institutions in the outbreak area until 21 days after the onset of rash in the last case of measles
Treatment
There is no specific antiviral therapy for measles
Supportive care to address symptoms and complications
Severe measles in children: Administer Vitamin A (a substrate for preserving epithelial cell integrity and involved in immune modulation) immediately on diagnosis and repeated the next day with following dosing
<6 months: 50,000 IU
6–11 months: 100,000 IU
≥12 months: 200,000 IU
Measles and Pregnancy
Pregnant women are considered a ‘high risk’ category due to increased risk for adverse maternal, fetal and newborn events
Maternal: Increased risk of hospitalization and severe respiratory complications including pneumonia
Fetal Alcohol Spectrum Disorders – CDC Summary and Updates
WHAT IS IT?
The current understanding of Fetal Alcohol Spectrum Disorder (FASD) is that there is no known safe amount of alcohol during pregnancy or when trying to get pregnant. All types of alcohol are equally harmful, including all wines and beer. Professional colleges recommend screening women in pregnancy. Fetal Alcohol Syndrome (FAS) is on the most severe end of the spectrum.
Smooth philtrum (ridge between nose and upper lip)
Thin vermillion (upper lip)
Small palpebral fissures (distance between inner and outer corners of the eyes) giving the eyes a wide-spaced appearance
Growth problems (prenatal or postnatal)
Height and/or weight ≤10th percentile
CNS
Structural
Head circumference ≤10th percentile
Clinically significant brain abnormalities observable through imaging
Neurological deficits unrelated to a postnatal insult or fever
Functional Performance below expectations
Global cognitive or intellectual deficits (Low IQ or developmental delay in younger children) or
Problems in at least 3 of the following areas
Cognitive or developmental deficits or discrepancies | Executive functioning deficits | Motor functioning delays | Attention deficit or hyperactivity | Social skills | Other problems such as sensory / language / memory
Maternal Alcohol Exposure
Helpful if maternal alcohol use can be confirmed during pregnancy
Confirmation of maternal alcohol use is not needed if child meets the other, above criteria
CNS, cognitive and behavioral effects without growth restriction and typical facial experience
Intellectual disabilities | Behavior and Learning abnormalities
Difficulties with math, memory, attention, judgment and impulse control
Requires confirmation of prenatal alcohol exposure
Alcohol-Related Birth Defects (ARBD)
Abnormal physical findings only (see more detail below in ‘Key Points’)
Heart | Kidneys | Bones | Hearing
Requires confirmation of prenatal alcohol exposure
Neurobehavioral Disorder Associated with Prenatal Alcohol Exposure (ND-PAE)
ND-PAE was first included as a recognized condition in the Diagnostic and Statistical Manual 5 (DSM 5) of the American Psychiatric Association (APA) in 2013
Problems identified
Thinking and memory, where the child may have trouble planning or may forget material he or she has already learned
Behavior problems, such as severe tantrums, mood issues (for example, irritability), and difficulty shifting attention from one task to another
Trouble with day-to-day living, which can include problems with bathing, dressing for the weather, and playing with other children.
Diagnosis requires
>13 alcoholic drinks per month (30-day period) of pregnancy or
> 2 alcoholic drinks in one sitting
KEY POINTS:
Structural abnormalities associated with prenatal alcohol exposure include
Facial abnormalities (described above plus short nose, cleft lip/palate)
Cardiac anomalies (ASD, VSD, abnormal great vessels)
In October 2017, the FDA approved and ACIP recommended a Shingrix (RZV) vaccine for adults ≥50 years of age. Zostavax (ZVL) is no longer available for use in the United States, as of November 18, 2020.
Herpes zoster is a localized, painful, cutaneous eruption resulting from reactivation of latent varicella zoster virus (VZV)
Approximately one million cases occur each year in the United States
Incidence increases with age
50 to 59 years of age: 5 cases per 1,000
≥80 years: 11 cases per 1,000
Postherpetic Neuralgia is the most common complication
Defined as persistent pain for at least 90 days following the resolution of the herpes zoster rash
Occurs in 10 to 13% of herpes zoster cases in persons aged >50 years and risk increases with age
Herpes Zoster Vaccine Recommendations
Shingrix is recommended for the prevention of herpes zoster and related complications for immunocompetent adults aged ≥50 years
Two doses of Shingrix provides strong protection against shingles and postherpetic neuralgia (PHN), the most common complication of shingles
Shingles Prevention: In adults 50 to 69 years old who got two doses, Shingrix was 97% effective; among adults 70 years and older, Shingrix was 91% effective
Postherpetic Neuralgia: In adults 50 to 69 years old who got two doses, Shingrix was 91% effective; among adults 70 years and older, Shingrix was 89% effective
Shingrix protection remained high (more than 85%) in people 70 years and older throughout the four years following vaccination
Shingrix is recommended for the prevention of herpes zoster and related complications for immunocompetent adults who previously received Zostavax or have already had herpes zoster
There is no maximum age for Shingrix
Clinical Guidance
Administer 2 doses (0.5 mL each) administered intramuscularly 2 to 6 months apart
Shingrix may be used in adults aged ≥50 years, irrespective of prior receipt of varicella vaccine or Zostavax
If patient previously received Zostavax
Consider the patient’s age and when he or she received Zostavax to determine when to vaccinate with Shingrix | Differences in efficacy between Shingrix and Zostavax are most pronounced among older patients
Studies examined the safety of Shingrix vaccination five or more years after Zostavax vaccination | Shorter intervals were not studied, but there are no theoretical or data concerns to indicate that Shingrix would be less safe or effective if administered less than five years after a patient received Zostavax
Screening for a history of chickenpox (varicella) not required
Recombinant and adjuvanted vaccines, such as Shingrix, can be administered concomitantly at the same visit, at different anatomic sites, with other adult vaccines (e.g., influenza and pneumococcal vaccines)
Shingrix is not a treatment for herpes zoster or postherpetic neuralgia
Pregnancy and breastfeeding
There are no available data to establish whether Shingrix is safe in pregnant or lactating women
Consider delaying vaccination with Shingrix in such circumstance
KEY POINTS:
Counseling and Adverse Events
Reactions to the first dose of Shingrix did not strongly predict reactions to the second dose
Vaccine recipients should be encouraged to complete the series even if they experienced a grade 1 to 3 reaction to the first dose of Shingrix
In studies, Grade 3 solicited symptoms were defined as “preventing normal everyday activity” (pain, headache, fatigue, gastrointestinal symptoms, myalgia, shivering) | surface diameter >100 mm (redness/swelling) | tympanic/oral/axillary temperature >39.0 °C (fever)
Grade 3 unsolicited adverse events were also defined as “preventing normal, everyday activities”
Adverse Events
The impact of prophylactic analgesics in conjunction with Shingrix has not been studied
Adverse local events are relatively common and include
Pain
Redness
Swelling
General adverse reactions include
Myalgia
Fatigue
Headache
Shivering
Fever
Gastrointestinal symptoms
Severe (rare) events include
Difficulty breathing
Wheezing
Hives
Pale skin
Fast heartbeat
Dizziness
Contraindications
History of severe allergic reaction (e.g., anaphylaxis) to any component of the vaccine ORafter previous dose
Acute episode of herpes zoster | Wait until acute episode has abated
Special Populations
Persons with a history of herpes zoster
Adults with a history of herpes zoster should receive Shingrix as herpes zoster can recur
Persons with chronic medical conditions (e.g., chronic renal failure, diabetes mellitus, rheumatoid arthritis, and chronic pulmonary disease)
Shingrix should be used
Immunocompromised persons
Shingrix may be used in persons taking low-dose immunosuppressive therapy (e.g., <20 mg/day of prednisone or equivalent or using inhaled or topical steroids), persons anticipating immunosuppression or who have recovered from an immunocompromising illness
Advisory Committee on Immunization Practices recommended 2 RZV doses for prevention of herpes zoster and related complications in immunodeficient or immunosuppressed adults aged ≥19 years
Second RZV dose should be given 2 to 6 months after the first | For persons who are or will be immunodeficient or immunosuppressed and who would benefit from a shorter vaccination schedule, the second dose can be administered 1 to 2 months after the first
Persons known to be VZV negative
Screening for a history of varicella (either verbally or via laboratory serology) is not recommended
However, in persons known to be VZV negative via serologic testing, ACIP guidelines for varicella vaccination should be followed
All healthy adults should be assessed for varicella immunity, and those who do not have evidence of immunity should receive 2 doses of single-antigen varicella vaccine 4-8 weeks apart
Shingrix has not been evaluated in persons who are VZV seronegative and the vaccine is not indicated for the prevention of chickenpox (varicella)
Cascade Testing: Notifying and Counseling Relatives of Individuals who are BRCA Mutation Carriers
CLINICAL ACTIONS:
Cascade testing is the process of identifying blood relatives of an individual with a potentially disease-causing mutation in genes such as BRCA1 or BRCA2 (see ‘Related ObG Topics’ below for summaries). Relatives may have inherited the same mutation and may also be at risk. Cascade testing is an efficient way of finding individuals who would benefit from counseling and genetic testing, if they so choose. If you have a patient who has received a report indicating that they are a carrier of a such a pathogenic variant, consider the following
Ensure the patient herself has obtained appropriate care and counseling
ACOG recommends that if a provider does not have the necessary genetic expertise, a referral should be made to genetic services and possibly medical and/or gynecologic oncologists
Any outreach to relatives of a patient should not come directly from the healthcare team without patient permission
Direct communication of your patient’s health information to a relative without permission may be in violation of HIPAA and/or state laws (see ‘Related ObG Topics’ below for more information)
Patients should be made aware that their findings may have significant consequences for other family members
ACOG states that tested patients “should be informed that they have a duty to notify relatives of the familial risk”
Be aware of potential barriers to family outreach by the patient including
The patient may be still be processing and making her own personal choices
There may be important family dynamics that need to be taken in to account
There may be logistical challenges such as knowing the location of family members
Financial concerns may delay or obstruct communication between patient and family due to worries regarding test reimbursement and medical costs
SYNOPSIS:
When someone has been identified as a carrier for a pathogenic mutation, there may be serious ramifications for blood relatives. Cascade testing has been shown to be a cost-effective and efficient way to identify other family members who may be at risk and make them aware of lifesaving options. HBOC and Lynch syndrome have been identified by the CDC as high priority syndromes for cascade testing. There are other genetic syndromes such as Familial Hypercholesterolemia where interventions can be lifesaving and cascade testing may be helpful to family members.
KEY POINTS:
Provide Support and Resources
Ensure patients have direct lines of communication to genetic counseling services if relatives, following notification, do want more information
Be aware of any ongoing state and professional programs that provide educational resources regarding genetic disorders, especially heritable cancer syndromes
ACOG provides a template for a letter that a provider can use to reach out to a family member following patient discussion/approval (see ACOG Committee Opinion in ‘Learn More – Primary Sources’ below)
Key highlights of relative communication include the following
Inform the family member as to the gene involved and the potential disorder
Explain that having a mutation does not necessarily always result in disease but it does mean that an individual who carries this variant is at higher risk
If providing overall lifetime risks for carriers, clarify that these are population based numbers and genetic counseling is required to personalize these risk figures
Apprise the family member that she may be a risk of having inherited this pathogenic mutation as well
In the case of autosomal dominant heritable cancer syndromes, that risk will be 50%
Clarify that aside from yourself, there are options including speaking to their own personal physician, a genetic counselor or other providers who may be of assistance
Good care requires a multi-disciplinary approach
Be prepared to share information about potential costs involved in genetic testing
Waive the Copay and Wave Hello to Potential Legal Penalties
To help out their patients burdened by healthcare costs, providers may on occasion consider not collecting copayments and deductibles. The patient may claim financial distress. Or the amount may not seem worth pursuing, although $20 or more per patient quickly adds up over the course of a year. Routinely waiving copays, however, makes you vulnerable to charges under the federal False Claims Act, as well as the federal antikickback law and similar state laws. And you risk fines of up to $25,000 and possible exclusion from federal insurance programs for violating the federal antikickback law alone.
Except in limited circumstances, Medicare and Medicaid don’t allow such waivers and demand that providers collect those amounts from patients. Routinely waiving them can be interpreted as program abuse. Why? Because a claim to government programs for patients in which a copayment or deductible was waived is misrepresenting the true charge for service. And there’s more. Rather than being perceived as the kindhearted person that you are, not collecting these payments can make it appear as if you are trying to attract patients by offering something of value, and consequently generating Medicaid or Medicare payments – a violation of the antikickback law.
If the patient has private insurance, you could be giving the patient’s insurer an opening to escape paying its share of your bill. For example, assume there is a $100 total charge where the patient has an 80/20 plan. If the provider waives the patient’s obligation to pay 20%, then, again arguably, the commercial plan owes only 80% of $80.
Be especially wary of copays. The rules of managed care are federally mandated and clearly state that the patient cannot see the doctor until they make their copayment. Many providers will recognize this clause in their contracts with insurance companies. Health insurance (including commerical) is also governed by a set of federal laws that fall under ERISA (The Employee Retirement Income Security Act). Commercial insurers can claim that the doctor interfered with their contracts with employers/individuals and some insurance companies have been aggressively fighting back on this front, including using the courts. Therefore, the safest course is simply to avoid granting copay waivers. If a patient has a true well-defined financial hardship, document the situation and in isolated, worthy cases, there is the option of reducing a deductible.
Ultimately, regardless of how onerous or convoluted insurance plans are, the responsibility for these payments rests with the patient as conceptually, they have entered into a ‘cost sharing’ arrangement with the company or organization that is providing their healthcare coverage.
IUDs and Implants: How to Manage Potential LARC Complications
Use of long-acting reversible contraceptive (LARC) methods, both intrauterine devices and subdermal contraceptive implants, has increased dramatically in the past ten years. Although the risk of complications is low, as use increases the absolute number of complications will increase.
CLINICAL ACTIONS:
Intrauterine device:
Pain
Lidocaine paracervical block reduces pain scores on insertion
Misoprostol does not improve pain scores and may be associated with nausea and vomiting
Strings not visualized
Rule out pregnancy and expulsion
Recommend backup contraception until IUD position can be verified
Ultrasound and X-ray of abdomen and pelvis can be used for localization
Possible expulsion
IUDs seen in the cervix are partially expelled and should be removed
Replacement or use of another method are both acceptable options
Low-lying IUDs (lower uterine segment) can be expectantly managed
Risk factors for expulsion include
Young age
Heavy menstrual bleeding and dysmenorrhea
Placement postpartum or post second trimester abortion
Presence of anatomic distortion of the uterine cavity
Uterine perforation
Is rare and generally asymptomatic
Usually occurs at the time of insertion
Do not use misoprostol routinely prior to insertion in nulliparous women but may be considered with difficult insertions
Rule out pregnancy and remove surgically unless the surgical risks of removal outweigh the benefits
PID
Can be treated with the IUD left in situ
Consider removal if no clinical improvement after 48-72 hours of antibiotics
Pregnancy with an IUD in place
Remove the IUD if the strings are visible or IUD within the cervix
IUD can be removed at time of procedure if patient elects termination
Evaluate for ectopic pregnancy
Implant:
Infection prevention
Use antiseptic technique and cover the insertion/removal site
Skin flora are the most common cause of infection
Remove implant if infection does not resolve
Bruising
Is common
Ice and anti-inflammatory medication can help
Nonpalpable implant
Locate with high frequency (>/= 10 MHz) ultrasound probe, two dimensional X-ray, or CT scan/fluoroscopy
Obtain a serum etonogestrel level if all studies are negative/equivocal
Refer to a surgeon with knowledge of the anatomy of the arm if implant is within muscle or neurovascular bundle
Pregnancy
Is rare
Remove the implant if the pregnancy is to be continued
Rule out ectopic pregnancy
SYNOPSIS:
LARCs are highly effective contraceptives with a low risk of complications. Those mentioned above should be discussed with patients as part of informed consent.
KEY POINTS:
Recognition and prompt diagnosis/treatment of the untoward outcomes described above are important aspects of care
Overall, complication rates are low and LARCs remain a very effective mode of birth control
OBG Project CME requires a modern web browser (Internet Explorer 10+, Mozilla Firefox, Apple Safari, Google Chrome, Microsoft Edge). Certain educational activities may require additional software to view multimedia, presentation, or printable versions of their content. These activities will be marked as such and will provide links to the required software. That software may be: Adobe Flash, Apple QuickTime, Adobe Acrobat, Microsoft PowerPoint, Windows Media Player, or Real Networks Real One Player.
Disclosure of Unlabeled Use
This educational activity may contain discussion of published and/or investigational uses of agents that are not indicated by the FDA. The planners of this activity do not recommend the use of any agent outside of the labeled indications.
The opinions expressed in the educational activity are those of the faculty and do not necessarily represent the views of the planners. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications, and warnings.
Disclaimer
Participants have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional development. The information
presented in this activity is not meant to serve as a guideline for patient management. Any procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this activity should not be used by clinicians without evaluation of their patient’s conditions and possible contraindications and/or dangers in use, review of any applicable manufacturer’s product information, and comparison with recommendations of other authorities.
Jointly provided by
NOT ENOUGH CME HOURS
It appears you don't have enough CME Hours to take this Post-Test. Feel free to buy additional CME hours or upgrade your current CME subscription plan
You are now leaving the ObG website and on your way to PRIORITY at UCSF, an independent website. Therefore, we are not responsible for the content or availability of this site