Key Highlights from the ASCCP Management Consensus Guidelines for Abnormal Cervical Cancer Screening Results
SUMMARY:
ASCCP guidance informs the assessment and treatment of abnormal cervical cancer screening results. The overarching theme of the recommendations reflects a ‘risk-based’ strategy, rather than rigid focus on a particular result. Risk tables have been generated to assist the clinician and guide practice. This is a consensus document with input from ACOG, ACS, SGO and multiple other professional organizations, including those affiliated with laboratory medicine.
The executive summary states
New data indicate that a patient’s risk of developing cervical precancer or cancer can be estimated using current screening test results and previous screening test and biopsy results, while considering personal factors such as age and immunosuppression
For a given current results and history combination, the immediate CIN 3+ risk is examined
If this risk is 4% or greater, immediate management via colposcopy or treatment is indicated
If the immediate risk is less than 4%, the 5-year CIN 3+ risk is examined to determine whether patients should return in 1, 3, or 5 years
Routine screening applies only to asymptomatic individuals who do not require surveillance for prior abnormal screening results
KEY POINTS:
Recommendations (colposcopy and treatment vs surveillance) are based on risk for CIN 3+
Risk determined by prior history as well as screen results
Risk tables also address ‘unknown history’ scenario
Deferral of colposcopy: Low risk for CIN 3+ (risk defined by tables)
Repeat HPV testing or cotesting at 1 year
At the 1-year follow-up test, referral to colposcopy if still abnormal
Expansion of expedited treatment category (biopsy not needed prior to therapy), for example, in nonpregnant patients ≥25 years, expedited treatment is
Preferred: CIN 3+ risk is ≥60%
Preferred: HPV 16–positive HSIL cytology and never or rarely screened patients with HPV-positive HSIL regardless of HPV genotype
Acceptable: CIN 3+ risk is between 25% and 60%
Shared decision making is important in the context of “impact on pregnancy outcomes”
Excisional treatment
Preferred over ablation for HSIL (CIN 2 or CIN 3) in the US
Recommended for AIS
CIN 1
Observation is preferred vs treatment
Treatment acceptable with persistent CIN 1 results >2 years
Lower Anogenital Squamous Terminology (LAST)/World Health Organization (WHO) recommendations for reporting histologic HSIL
Include HSIL (CIN 2) and HSIL (CIN 3) (i.e., include CIN 2 and 3 qualifiers)
Reflex cytology
Should be performed on all positive HPV tests, regardless of genotype
If HPV 16 and 18 testing is positive but additional laboratory testing of the same sample is not feasible, proceed directly to colposcopy
Surveillance recommendations following histologic HSIL, CIN 2, CIN 3, or AIS
Continue surveillance with HPV testing or cotesting at 3-year intervals for at least 25 years (recommended)
>25 years is acceptable “for as long as the patient’s life expectancy and ability to be screened are not significantly compromised by serious health issues”
HPV assays
The ASCCP consensus document states the following in reference to HPV tests
Human papilloma virus assays that are Food and Drug Administration (FDA)-approved for screening should be used for management according to their regulatory approval in the United States
Note: All HPV testing in this document refers to testing for high-risk HPV types only
For all management indications, HPV mRNA and HPV DNA tests without FDA approval for primary screening alone should only be used as a cotest with cytology, unless sufficient, exceptionally rigorous data are available to support primary HPV testing in management
Trichomoniasis: CDC Diagnosis and Treatment Guidelines
SYNOPSIS:
Trichomoniasis is the most prevalent nonviral sexually transmitted infection worldwide.The U.S. population-based T. vaginalisprevalence is 2.1% among females and 0.5% among males, with the highest rates among Black females (9.6%) and Black males (3.6%), compared with non-Hispanic White women (0.8%) and Hispanic women (1.4%)The majority of persons who have trichomoniasis (70%–85%) either have minimal or no genital symptoms, and untreated infections might last from months to years, however, data are lacking on whether screening and treatment for asymptomatic trichomoniasis is beneficial. Decisions about screening might be informed by local epidemiology of T. vaginalis infection rates.
CLINICAL ACTIONS:
Male: Urethritis| Epididymitis | Prostatitis
Women: Vaginal Discharge| Vulvar Irritation
Diagnostic testing for T. vaginalis should be performed in women seeking care for vaginal discharge (yellow-green, with or without irritation). Screening might be considered for women receiving care in high-prevalence settings.
Diagnosis
Perform nucleic acid amplification testing (NAAT), which detects T. vaginalis genetic material, is highly sensitive and which is three to five times more likely to identify T. vaginalis infections than wet-mount microscopy, a method with poor sensitivity
Culture was considered the gold standard before molecular testing and is less sensitive than newer tests
If wet preparations are used, despite lower sensitivities, slides should be evaluated immediately as sensitivity declines with time
If negative, consider follow up with a NAAT to make sure infection is truly not present
T. vaginalis may be an incidental finding on a Pap test, neither conventional nor liquid-based Pap tests are considered diagnostic tests for Trichomoniasis, because false negatives and false positives can occur
KEY POINTS:
The nitroimidazoles are the only class of antimicrobial medications known to be effective against T. vaginalis infections. Of these drugs, metronidazole and tinidazole have been cleared by FDA for the oral or parenteral treatment of trichomoniasis.
The CDC recommends the following
Women
Metronidazole 500 mg 2 times/day for 7 days
Men
Metronidazole 2 g orally in a single dose
Alternative regimen for men and women
Tinidazole 2 g orally in a single dose
Note: ACOG also recommends metronidazole 500 mg orally twice a day for 7 days as the recommended treatment option with tinidazole, 2 g orally in a single dose as the alternative regimen
Alcohol consumption should be avoided during treatment with nitroimidazoles
To reduce the possibility of a disulfiram-like reaction, abstinence from alcohol use should continue for 24 hours after completion of metronidazole or 72 hours after completion of tinidazole
Providers should advise persons infected with T. vaginalis to abstain from sex until they and their sex partners are treated (i.e., when therapy has been completed and any symptoms have resolved)
Testing for other STDs including HIV should be performed in persons infected with T. vaginalis
Retest for T. vaginalis is recommended for all sexually active women within 3 months following initial treatment
Testing by NAAT can be conducted as soon as 2 weeks after treatment
Treat current partners to avoid reinfection and further transmission
Partners should be advised to abstain from intercourse until they and their sex partners have been adequately treated and any symptoms have resolved
In States where legally allowed (see learn more below), consider Expedited Partner Therapy (EPT) which allows the patient herself to provide medications to her partner when there are limited public health services to treat a partner, or concern that the partner will not have access to treatment
Pregnancy
T. vaginalis infection is associated with two to threefold increased risk for HIV acquisition, preterm birth, and other adverse pregnancy outcomes among pregnant women
However, some trials have not shown improvement in perinatal morbidity with treatment
Symptomatic pregnant women, regardless of pregnancy stage, should be tested and considered for treatment with metronidazole
Tinidazole should be avoided for pregnant women
The benefit of routine screening for T. vaginalis in asymptomatic pregnant women has not been established
HIV
Among women with HIV infection, up to 53% are also infected with T. vaginalis which has been associated with an increased risk for PID
Routine screening of asymptomatic women with HIV infection for T. vaginalis is recommended on entry to care, and then annually
Pregnant women, including those who are asymptomatic, should be screened and treated as necessary because T. vaginalis infection is a risk factor for vertical HIV transmission
The recommended regimen in the setting of HIV is as follows
Chlamydia: CDC Recommendations for Diagnosis and Treatment
CLINICAL ACTIONS:
Annual screening of all sexually active women aged <25 years for chlamydia is recommended, as is screening of older women at increased risk for infection (e.g., those who have a new sex partner, more than one sex partner, a sex partner with concurrent partners, or a sex partner who has an STD).
To diagnose a chlamydia infection:
Obtain nucleic acid amplification testing (NAAT), which detects genetic material of C. trachomatis
Highly sensitive in first-catch urine samples and endocervical or vaginal swabs
Can be collected by a provider or a self-collected vaginal swab
Certain NAATs have been FDA-cleared for use on liquid-based cytology specimens (collected for Pap smears), however sensitivity may be lower than swabs
SYNOPSIS:
Chlamydial infection is the most frequently reported infectious disease in the United States, and prevalence is highest in persons aged ≤24 years. Several sequelae can result from C. trachomatis infection in women, the most serious of which include PID (pelvic inflammatory disease), ectopic pregnancy, and infertility. Some women who receive a diagnosis of uncomplicated cervical infection already have subclinical upper-reproductive–tract infection.
KEY POINTS:
Chlamydia treatment should be provided promptly for all persons testing positive for infection; treatment delays have been associated with complications
Recommended Regimens
Azithromycin 1 g orally in a single dose or
Doxycycline 100 mg orally twice a day for 7 days
Alternative Regimens
Erythromycin base 500 mg orally four times a day for 7 days or
Erythromycin ethylsuccinate 800 mg orally four times a day for 7 days or
Levofloxacin 500 mg orally once daily for 7 days or
Ofloxacin 300 mg orally twice a day for 7 days
Routine pharyngeal screening for chlamydia is not recommended, but if C. trachomatis is detected in an oropharyngeal specimen treat with azithromycin or doxycycline
Directly observe patient receiving therapy when single dose therapy is given
To minimize disease transmission to sex partners, persons treated for chlamydia should be instructed to abstain from sexual intercourse for 7 days after single-dose therapy or until completion of a 7-day regimen and resolution of symptoms if present
To minimize risk for reinfection, patients also should be instructed to abstain from sexual intercourse until all of their sex partners are treated
Persons who receive a diagnosis of chlamydia should be tested for HIV, gonococcal infection, and syphilis
Test-of-cure to detect therapeutic failure is not advised unless therapeutic adherence is in question, symptoms persist, or reinfection is suspected
Chlamydial NAATs at <3 weeks after completion of therapy is not recommended because the continued presence of nonviable organisms can lead to false-positive results
Retest after 3 months
Recurrence may not be treatment failure but rather reinfection
In States where legally allowed (see ‘Related OBG Topics’ below), consider Expedited Partner Therapy (EPT) which allows the patient herself to provide medications to her partner when there are limited public health services to treat a partner, or concern that the partner will not have access to treatment
Treat women with HIV with the same recommended regimen
PREGNANCY AND CHLAMYDIAL INFECTION
Risks in pregnancy include preterm labor, premature rupture of membranes and low birth weight with neonates at risk for conjunctivitis (ophthalmia neonatorum) and pneumonia. It is therefore imperative to screen and treat pregnant women with the following:
Recommended Regimens
Azithromycin 1 g orally in a single dose
Alternative Regimens
Amoxicillin 500 mg orally three times a day for 7 days or
Erythromycin base 500 mg orally four times a day for 7 days or
Erythromycin base 250 mg orally four times a day for 14 days or
Erythromycin ethylsuccinate 800 mg orally four times a day for 7 days or
Erythromycin ethylsuccinate 400 mg orally four times a day for 14 days
Test-of-cure (preferably by NAAT) recommended at 3 to 4 weeks after completion of therapy and again after 3 months
Diagnosis code: Chlamydia: A74.9 (pregnant) or A56.02 (nonpregnant)
Bacterial Vaginosis – CDC Diagnosis and Treatment Recommendations
CLINICAL ACTIONS:
Bacterial Vaginosis (BV) occurs when normal hydrogen peroxide producing Lactobacillus sp. is replaced by an overgrowth of facultative anaerobic bacteria. If a woman presents with symptoms, including vaginal discharge, irritation and malodor
Diagnose BV if 3 of the following (Amsel) clinical criteria are present
Homogeneous, thin, white discharge that smoothly coats the vaginal walls
More than 20% clue cells (e.g., vaginal epithelial cells studded with adherent coccobacilli) on saline microscopic examination
pH of vaginal fluid >4.5
Fishy odor of vaginal discharge before or after addition of 10% KOH (i.e., the whiff test), OR
Gram stain with Nugent scoring is considered the gold standard to diagnose
Used in research settings; impractical for clinicians so Amsel criteria preferred clinically
Assigns a score to various bacterial concentrations seen on gram stain: 0-3 Normal | 4-6 Intermediate | 7-10 Bacterial vaginosis
Affirm VP III (Becton Dickinson, Sparks, MD), a DNA hybridization probe test for high concentrations of G.vaginalis
OSOM BV Blue test (Sekisui Diagnostics, Framingham, MA), which detects vaginal fluid sialidase activity, have acceptable performance characteristics compared with Gram stain
Nucleic Acid Amplification Tests (NAAT) are also available and “can be used as an alternative to clinical testing in settings where pH paper, KOH, and microscopy are not available”
Do NOT use Pap tests
Do NOT culture for G. vaginalis given normal vaginal flora is heterogenous
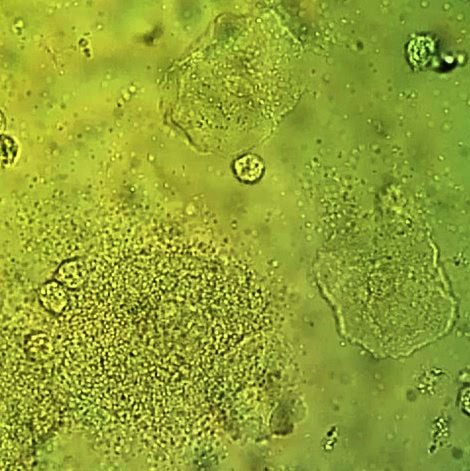
Vaginal wet mount with a NaCl preparation, showing a clue cell at bottom left, and two normal epithelial cells.
SYNOPSIS:
Bacterial Vaginosis (BV) is not caused by a single bacterium, but by high concentrations of facultative anaerobic bacteria (e.g., Prevotella sp. and Mobiluncus sp.), G. vaginalis, Ureaplasma, Mycoplasma, and numerous other anaerobes. BV is associated with multiple or new sex partners, lack of condom use and in particular lack of vaginal lactobacillus. Because BV is not an inflammatory condition, vulvar erythema and edema are not commonly seen, unlike candidiasis and trichomoniasis.
KEY POINTS:
Treatment is recommended for women with symptoms, including discharge, irritation and malodor and may reduce the risk for C. trachomatis, N. gonorrhoeae, T. vaginalis, HIV, and herpes simplex type 2.
Recommended CDC regimens include the following:
Metronidazole* 500 mg orally twice a day for 7 days OR
Metronidazole* gel 0.75%, one full applicator (5 g) intravaginally, once a day for 5 days OR
Clindamycin** cream 2%, one full applicator (5 g) intravaginally at bedtime for 7 days
Alternative Regimens
Tinidazole* 2 g orally once daily for 2 days OR
Tinidazole* 1 g orally once daily for 5 days OR
Clindamycin** 300 mg orally twice daily for 7 days OR
Clindamycin** ovules 100 mg intravaginally once at bedtime for 3 days
Secnidazole 2 g orally in a single dose
*Alcohol consumption should be avoided during treatment with oral nitroimidazoles. To reduce the possibility of a disulfiram-like reaction, abstinence from alcohol use should continue for 24 hours after completion of metronidazole and 72 hours after completion of tinidazole.
**Clindamycin ovules use an oleaginous base that might weaken latex or rubber products (e.g., condoms and vaginal contraceptive diaphragms). Use of such products within 72 hours following treatment with clindamycin ovules is not recommended.
Test all women with BV for HIV and other sexually transmitted diseases (STDs)
Follow-up visits are unnecessary if symptoms resolve
Routine treatment of sex partners in not recommended
Using a different recommended treatment regimen can be considered in women who have a recurrence
Retreatment with the same recommended regimen is an acceptable approach for treating persistent or recurrent BV after the first occurrence
Recurrent BV: At least 3 documented, separate episodes of BV in one year
0.75% metronidazole gel twice weekly for 4–6 months has been shown to reduce recurrences, although this benefit might not persist when suppressive therapy is discontinued
BV and Preterm Birth
The USPSTF addresses BV screening during pregnancy and states the following
The USPSTF recommends against screening for bacterial vaginosis in pregnant persons not at increased risk for preterm delivery. (D recommendation)
The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for bacterial vaginosis in pregnant persons at increased risk for preterm delivery. (I statement)
Pregnant women are considered a ‘special population’ by the CDC. Due to the potential burden to pregnant women, offspring and partners, providers should ask all pregnant women and their partners about STIs, and ensure counseling, screening and treatment are available.
Rapid HIV testing should be performed on any woman in labor who has not been screened during pregnancy, unless she declines
If rapid HIV test positive, antiretroviral prophylaxis should be administered prior to receiving confirmatory test results
AAP recommends expedited HIV testing as soon as possible after birth for infants born to women with unknown HIV status
NOTE: The USPSTF (June 2019) continues to recommend screening for HIV infection in all pregnant persons, including those who present in labor or at delivery whose HIV status is unknown. (A recommendation)
SYPHILIS
Cases of congenital syphilis have increased 10 fold in the past decade
Syphilis during pregnancy can lead to
Stillbirth | Miscarriage | Infant death | Maternal and infant morbidity
Serologic tests should be performed at first prenatal visit
Screening for syphilis infection is a 2-step process | Antepartum screening can be performed by manual nontreponemal antibody testing (e.g., RPR) by using the traditional syphilis screening algorithm or by treponemal antibody testing (e.g., immunoassays)
Traditional screening
Initial “nontreponemal” antibody test (ie, Venereal Disease Research Laboratory test or rapid plasma reagin [RPR] test) to detect biomarkers released from damage caused by syphilis infection
Followed by a confirmatory “treponemal” antibody detection test (ie, fluorescent treponemal antibody absorption [FTA-ABS] or T pallidum particle agglutination test [TP-PA])
Reverse sequence screening algorithm
Initial automated treponemal test (such as an enzyme-linked [EIA], chemiluminescence [CIA], or multiplex flow immunoassay [immunoblot])
Followed by a nontreponemal test
NOTE: If the test results of the reverse sequence algorithm are discordant, a second treponemal test (preferably using a different treponemal antibody) is performed
Pregnant women with positive treponemal screening tests (e.g., EIA, CIA, or immunoblot) should have additional quantitative nontreponemal testing because titers are essential for monitoring treatment response
If access to prenatal care is suboptimal, RPR test and treatment should be performed at time of pregnancy confirmation
Serologic retesting in the 3rd trimester (28 weeks) and at delivery if the patient for patients at high risk including
Sex with multiple partners | Sex in conjunction with drug use or transactional sex
Late entry to prenatal care (i.e., first visit during the second trimester or later) or no prenatal care
Methamphetamine or heroin use
Incarceration of the woman or her partner
Unstable housing or homelessness
Test any woman who delivers a stillborn or in the case of infant death
Untreated syphilis has a 40% infant death rate
Do NOT discharge neonate if serologic status is unknown
Newborn infection may not be immediately obvious
Within a few weeks may develop
Developmental delay
Seizures
Birth defects such as bone deformation, blindness and deafness
Note: In September 2018, the USPSTF reaffirmed previous guidance and “recommends early screening for syphilis infection in all pregnant women.” (Grade A – Offer or Provide this Service)
HEPATITIS B (HBV)
Screen during each pregnancy, preferably in the first trimester, regardless of vaccination status or history of testing
Use ‘triple panel’: Hepatitis B surface antigen (HBsAg), antibody to HBsAg, and total antibody to HBcAg (total anti-HBc)
If patient underwent appropriately timed triple panel screening and has not had any new HBV exposures since triple panel screening, only HBsAg screening is required
At time of admission for delivery, retest if patient
Is at high risk – more than one sex partner in previous 6 months, evaluation or treatment for STI, injection-drug use, HBsAG-positive sex partner
Was not screened prenatally
Has clinical hepatitis
Always do HBsAg testing prior to giving the HBV vaccine to avoid misinterpretation
Report HBsAg positive women to local or state health departments to ensure they are entered into a case management program to arrange access to appropriate vaccinations for contacts and prophylaxis for infants
If HBsAg positive, test for hepatitis B virus deoxyribonucleic acid (HBV DNA) to guide the use of antiviral medication to prevent perinatal transmission
If HBV DNA >200,000 IU/mL (7.6 log10 IU/mL): The American Association for the Study of Liver Diseases suggests antiviral therapy during pregnancy to further reduce perinatal HBV transmission
HEPATITIS C (HCV)
The CDC has updated HepC guidelines (2020)
Hepatitis C screening at least once in a lifetime for all adults aged ≥18 years, except in settings where the prevalence of HCV infection (HCV RNA-positivity) is <0.1%
Hepatitis C screening for all pregnant women during each pregnancy, except in settings where the prevalence of HCV infection (HCV RNA-positivity) is <0.1%
USPSTF also calls for universal screening for HCV infection, including pregnancy
Recommended Screening Tests for Pregnant Women at Risk
CHLAMYDIA
Test all pregnant women who are <25 years old for Chlamydia trachomatis at the first prenatal visit
Test all older women if at high risk:
More than one sex partner
A sex partner with concurrent partners or has an STI
Retest in the 3rd trimester to prevent maternal postnatal complications and chlamydia infection in the neonate
Test of cure by NAAT 3 to 4 weeks after treatment and retest within 3 months
GONORRHEA
Test all pregnant women who are <25 years old for N. gonorrhoeae at the first prenatal visit
Test all older women if at high risk:
More than one sex partner
A sex partner with concurrent partners or has an STI
Inconsistent condom use in non-monogamous relationships
Previous or co-existing sexually transmitted infections
Exchanging sex for money or drugs
Consider consulting local public health authorities for further guidance on identifying those at high risk related to geographic location
Treat all positive patients immediately and retest in 3 months
Retest in the 3rd trimester to prevent maternal postnatal complications and chlamydia infection in the neonate
Screen Only if Symptomatic
Bacterial Vaginosis (BV)
Evidence does not support routine screening
Evaluate and screen symptomatic women
The USPSTF addresses BV screening during pregnancy and states the following
The USPSTF addresses BV screening during pregnancy and states the following The USPSTF recommends against screening for bacterial vaginosis in pregnant persons not at increased risk for preterm delivery. (D recommendation)
The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for bacterial vaginosis in pregnant persons at increased risk for preterm delivery. (I statement)
Trichomonas
Evidence does not support routine screening
Evaluate and screen symptomatic women
HSV-2
Evidence does not support routine screening
In the absence of lesions during the 3rd trimester, routine cultures for HSV are not indicated for women in the 3rd trimester who have a history of recurrent genital herpes
Type-specific serologic tests may help identify pregnant women at risk for HSV and to help guide counseling regarding the risk of acquiring herpes during pregnancy
SYNOPSIS:
Recommendations for STI testing can vary based on certain considerations, including state laws. The CDC recommendations are considered broader, such that more women will potentially be screened, but are consistent with other CDC guidance with the intention of preventing adverse outcomes for pregnant women, partners and fetuses.
KEY POINTS:
All pregnant women and their partners should be asked about STIs and counseled regarding personal risks as well as pregnancy and outcomes
Pap Smears should be performed in pregnancy at the same frequency as nonpregnant women
Management of abnormal Pap tests differ in pregnancy
Screening at Delivery
SYPHILIS
Select groups of pregnant women, including women who are at high risk for syphilis or live in areas of high syphilis morbidity
Pregnant women with no previously established status
Pregnant women who deliver a stillborn infant
HIV
Pregnant women not screened during pregnancy
HBV
Women admitted for delivery at a health care facility without documentation of HBsAg test results should have blood drawn and tested as soon as possible after admission
Women at high risk
Having had more than one sex partner during the previous 6 months, an HBsAg-positive sex partner, evaluation or treatment for a sexually transmitted disease, or recent or current injection-drug use
Women with signs or symptoms of hepatitis
Note: CDC recommends universal hepatitis B vaccination within 24 hours of birth for medically stable infants >2000 grams
Permissive language that allowed the vaccine to be delayed until after hospital discharge has been removed
Administer hepatitis B vaccination and hepatitis immune globulin regardless of birth weight within 12 hours of birth for infants born to hepatitis b-infected mothers
CHLAMYDIA
Pregnant women less than 25 years of age
Continued high risk
New or multiple sex partners, sex partner with concurrent partners, sex partners who have a sexually transmitted disease
GONORRHEA
Continued high risk
Past or current injection-drug use, having had a blood transfusion before July 1992, receipt of an unregulated tattoo, having been on long-term hemodialysis, intranasal drug use, and other percutaneous exposures
Guidance Update: Professional Organizations Align on Cervical Cancer Screening
SUMMARY:
ACOG has joined ASCCP and the SGO in endorsing the USPSTF cervical cancer screening recommendations. The ACOG practice document states that
Consistent with prior guidance, screening should begin at age 21 years, and screening recommendations remain unchanged for average-risk individuals aged 21–29 years and those who are older than 65 years
Management of abnormal cervical cancer screening results should follow current ASCCP guidelines
CLINICAL ACTIONS:
The USPSTF recommends the following (Grade A – “Offer or Provide this Service”)
Begin screening at age 21
Screen every 3 years with cytology alone
Do not perform HPV testing routinely
Age 30 to 65 can be screened
Every 5 years ‘cotesting’ with cytology plus HPV
Every 3 years with cytology only
every 5 years with high-risk human papillomavirus (hrHPV) testing alone
The USPSTF recommends against the following (Grade D – Discourage the use of this service)
<21 years
Do not offer screening
>65 years
Do not offer screening in the setting of adequate prior screening and otherwise not at high risk for cervical cancer
Do not offer screening following hysterectomy if
Cervix was removed and
There is no history of a high-grade precancerous lesion (ie, cervical intraepithelial neoplasia [CIN] grade 2 or 3) or cervical cancer
SYNOPSIS:
Cervical cancer rates in the United States are low due largely to access to effective screening. Cervical cancer is believed with a high degree of certainty, to be the delayed consequence of infection with high risk or oncogenic human papillomavirus (HPV). The majority of HPV infections are transient and do not progress to cervical cancer. However, the consequences of missing precancerous or early cancerous lesions are potentially lethal and should be avoidable with appropriate screening.
KEY POINTS:
The goal of cervical cancer screening is to minimize harm and maximize benefit
Guidelines focus on increasing the age at which to begin screening, lengthening the screening interval and discontinuing screening women at low risk for future cervical cancer
The above action items refer to average risk women
Women at increased risk for cervical cancer require a higher level of surveillance and include those who are
Immunocompromised (HIV positive, organ transplant recipient, chronic steroid use)
Sex workers
Women with multiple partners or high risk partners
Women with a history of abnormal Pap smear or precancerous genital conditions
Smokers
Women with a history of sexually transmitted diseases
ACOG has responded to the American Cancer Society (2020) recommendation that hrHPV testing in isolation every 5 years should be prioritized for women 25 to 65 years of age
hrHPV alone has demonstrated efficacy and efficiency
However, the ACOG Practice Advisory notes significant limitations regarding current healthcare infrastructure, including
Limited access to primary hrHPV testing is of particular concern in rural and under-resourced communities and among communities of color, which have disproportionately high rates of cervical cancer incidence, morbidity, and mortality
Although HPV self-sampling has the potential to greatly improve access to cervical cancer screening, and there is an increasing body of evidence to support its efficacy and utility, it is still investigational in the United States
OBG Project CME requires a modern web browser (Internet Explorer 10+, Mozilla Firefox, Apple Safari, Google Chrome, Microsoft Edge). Certain educational activities may require additional software to view multimedia, presentation, or printable versions of their content. These activities will be marked as such and will provide links to the required software. That software may be: Adobe Flash, Apple QuickTime, Adobe Acrobat, Microsoft PowerPoint, Windows Media Player, or Real Networks Real One Player.
Disclosure of Unlabeled Use
This educational activity may contain discussion of published and/or investigational uses of agents that are not indicated by the FDA. The planners of this activity do not recommend the use of any agent outside of the labeled indications.
The opinions expressed in the educational activity are those of the faculty and do not necessarily represent the views of the planners. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications, and warnings.
Disclaimer
Participants have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional development. The information
presented in this activity is not meant to serve as a guideline for patient management. Any procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this activity should not be used by clinicians without evaluation of their patient’s conditions and possible contraindications and/or dangers in use, review of any applicable manufacturer’s product information, and comparison with recommendations of other authorities.
Jointly provided by
NOT ENOUGH CME HOURS
It appears you don't have enough CME Hours to take this Post-Test. We no longer offer Hours.
Leaving ObG Website
You are now leaving the ObG website and on your way to PRIORITY at UCSF, an independent website. Therefore, we are not responsible for the content or availability of this site