For both ‘vigorous’ term and preterm infants, ACOG recommends waiting at delayed clamping the umbilical cord. The committee opinion provides a comprehensive literature and evidence review. ACOG states
In term infants, delayed umbilical cord clamping increases hemoglobin levels at birth and improves iron stores in the first several months of life, which may have a favorable effect on developmental outcomes
Delayed umbilical cord clamping is associated with significant neonatal benefits in preterm infants, including improved transitional circulation, better establishment of red blood cell volume, decreased need for blood transfusion, and lower incidence of necrotizing enterocolitis and intraventricular hemorrhage
Benefits include
Term infants
Increased hemoglobin levels and iron stores
Preterm infants
Improved transitional circulation
Better establishment of RBC volume
Decreased blood transfusion
Lower risk of NEC and IVH
Note: There was no evidence for increased risk of PPH
Caution: The committee opinion notes that there may be a small risk for jaundice requiring phototherapy in term infants and therefore the delivery center should have the necessary infrastructure to monitor and treat, if necessary
Duration of Delay
Term
30 to 60 seconds
Preterm (See ACOG Update in ‘Learn More – Primary Sources’ below)
<37 weeks (no need for immediate resuscitation): ≥60 seconds
Maternal hemodynamic instability or the need for immediate resuscitation of the newborn on the warmer would be an indication for immediate umbilical cord clamping
Cord Milking
Based on the latest evidence (see ‘Learn More – Primary Sources’ ACOG Update below)
In preterm neonates born at 28 0/7–36 6/7 weeks of gestation who do not receive deferred cord clamping, umbilical cord milking is a reasonable alternative to immediate cord clamping to improve neonatal hematologic outcomes
Eclampsia is a severe, life-threatening manifestation of preeclampsia. While long-term neurologic damage is rare, there is risk of maternal hypoxia and death. Most women will experience signs such as headaches or visual changes prior to a seizure.
Eclampsia
Defined as convulsions during pregnancy and/or postpartum
Tonic-clonic, focal, or multifocal
New onset
Unexplained by other neurologic pathology
Consider other underlying cerebral conditions when
Seizures occur 2 to 3 days postpartum
Patient on magnesium sulfate
Note: Not all women will demonstrate classic features of preeclampsia (hypertension, proteinuria)
Magnesium Sulfate – How to Use
Magnesium sulfate is the treatment of choice for seizure prophylaxis (ACOG recommended dosing)
Loading dose of 4–6 g of magnesium sulfate administered per infusion pump over 20–30 minutes (i.e., slowly) followed by a maintenance dose of 1-2 g per hour as a continuous intravenous infusion
Continue 24 hours postpartum
Recurrent seizures
Additional dose of 2-4 g can be infused over 5 minutes
Refractory seizures
Sodium amobarbital: 250 mg IV in 3 minutes
Thiopental or phenytoin: 1,250 mg IV at a rate of 50 mg/minute
Patient should be managed in ICU
Consider neuroimaging
IM option
10 g initially as a loading dose (5 g IM in each buttock) followed by 5 g every 4 hours
Use if IV access limited
Mix with 1 mL xylocaine 2% to alleviate pain
Note: Magnesium sulfate should not be considered an antihypertensive agent
Magnesium Sulfate – When to Use
Severe features of preeclampsia
Administer to all women
No severe features of preeclampsia and systolic BP > 140 and < 160 mm Hg or diastolic BP > 90 and < 110 mm Hg
There is no consensus on this matter as prophylaxis will reduce eclampsia but 1 in 100 to 129 women need to be treated and side effects (although not life threatening) will increase
ACOG states that the decision to use magnesium sulfate when severe features are not present should be the decision of the “physician or institution, considering patient values or preferences, and the unique risk-benefit trade-off of each strategy”
Delivery and Postpartum
Vaginal delivery
Continue infusion 24 hours postpartum
Cesarean
Begin infusion (if not yet running) before surgery and continue 24 hours postpartum
Discontinuing prior to operative vaginal birth or cesarean section to avoid uterine atony or anesthetic drug interactions is not recommended
Prevention of Magnesium Sulfate toxicity
Place Foley to monitor renal function (hourly output)
Confirm normal serum creatinine
Serial evaluation of patellar deep tendon reflexes
Monitor respiratory rate
Serum magnesium levels not routinely required
Monitor serum magnesium levels in setting of renal dysfunction and/or absence of patellar reflexes
Maintain serum concentrations 5 to 9 mg/dL (4–7 mEq/L) range
Predictive symptoms of magnesium sulfate toxicity
Loss of deep tendon reflexes >9 mg/dL (greater than 7 mEq/L)
Respiratory depression >12 mg/dL (greater than 10 mEq/L)
Cardiac arrest >30 mg/dL (greater than 25 mEq/L)
Pending toxicity
Notify appropriate health care provider
Discontinue magnesium infusion
Administer supplemental oxygen
Obtain a serum magnesium level
Reverse magnesium
10 mL of 10% calcium gluconate IV (1 g total) and over 3 min (i.e., slowly) to avoid hypotension and/or bradycardia
Calcium effect (competitively inhibits magnesium at neuromuscular junction) can wear off if magnesium level stays high
Furosemide may help increase urinary excretion
Respiratory arrest: Intubation and assisted ventilation as indicated
Other Prophylactic Agents
Magnesium sulfate is superior to diazepam, phenytoin and lytic cocktail (chlorpromazine, promethazine, pethidine) in reducing significantly the risk of seizure recurrence
Cochrane Review 2010: Magnesium sulfate reduced eclampsia compared to phenytoin (relative risk 0.08, 95% CI 0.01 to 0.60)
Morbidity related to pneumonia, mechanical ventilation and admission to an intensive care unit are significantly reduced with the use of magnesium sulfate compared with phenytoin
Magnesium sulfate does not cause maternal or newborn CNS depression
Diazepam or lorazepam does stop or shorten seizures, but risk of maternal apnea and/or cardiac arrest
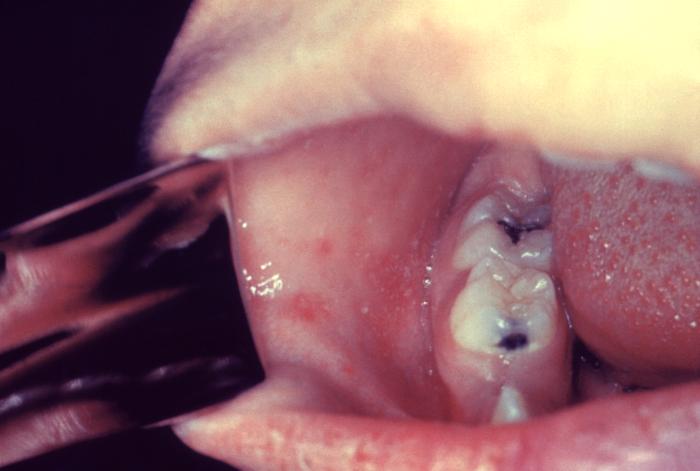
Otitis Media: 1/10 children and may result in permanent hearing loss
Severe complications in children requiring hospitalization
Acute encephalitis: 1/1,000 children, resulting in permanent brain damage
Respiratory and neurologic: 1/1,000 children will die from these complications
Subacute sclerosing panencephalitis (SSPE): Rare, fatal degenerative disease of CNS, resulting in deterioration and seizures 7 to 10 years after measles infection
Diagnosis and Testing
Clinical suspicion
Signs and symptoms detailed above
Special concern for those traveling internationally or exposed to someone with a febrile rash illness
Laboratory confirmation
Essential for all sporadic measles cases and all outbreaks
A capture IgM EIA (non-quantitative) that incorporates a recombinant measles nucleocapsid protein as the antigen is used to detect measles IgM
A commercial, indirect EIA (non-quantitative) assay is used to detect IgG
Viral detection methods: Includes real time RT-PCR to detect measles viral RNA | Available at many state public health laboratories and though the APHL/CDC Vaccine Preventable Disease Reference Centers (see ‘Learn More – Primary Sources’ below)
Detection of measles-specific IgM antibody in serum and measles RNA by RT-PCR in a respiratory specimen are the most common methods for confirming measles infection
Obtain both a serum sample and a throat swab (or nasopharyngeal swab) from patients suspected to have measles at first contact
Urine samples may also contain virus: If possible collect both respiratory and urine samples
Public Health: Molecular analysis (genotyping) can map transmission pathways of measles viruses
Evidence of Immunity
Note: Do not accept verbal reports of immunity
Acceptable presumptive evidence of immunity against measles includes ≥1 of the following
Written documentation of one or more doses of a measles-containing vaccine administered on or after the first birthday for preschool-age children and adults not considered high risk
Written documentation of two doses of measles-containing vaccine for school-age children and adults at high risk, including students at post-high school secondary educational institutions, healthcare personnel, and international travelers
Laboratory evidence of immunity *
Laboratory confirmation of measles
Birth before 1957
*Note: CDC addresses laboratory evidence of immunity and states the following
*People who have negative or equivocal results for measles IgG should be vaccinated or revaccinated. In some cases it is not possible to vaccinate a patient, and you may need to test them with a second line diagnostic assay to determine whether they are immune to measles. Because the sensitivity and specificity of commercial measles IgG assays vary, state public health departments can provide information on appropriate second line assays.
NOTE FOR HEALTHCARE PERSONNEL (HCP): CDC has interim guidance that states
Consider vaccinating HCP born before 1957 who do not have other evidence of immunity to measles
During a measles outbreak, 2 doses of measles virus-containing vaccine are recommended for all HCP, regardless of year of birth
See more HCP interim guidance using the CDC link below in ‘Learn More – Primary Sources’
Measles Vaccine Recommendations (CDC)
Children – MMR vaccine
First dose: 12 through 15 months of age
Second dose: 4 through 6 years of age no earlier than 28 days following the first dose
Students at post-high school educational institutions without evidence of measles immunity
2 doses of MMR vaccine
Second dose administered no earlier than 28 days after the first dose
Adults born ≥1957 who do not have evidence of measles immunity
Should get at least one dose of MMR vaccine
International travelers ≥6 months of age
Infants 6 through 11 months: one dose of MMR vaccine
One dose at 12 through 15 months of age and another dose at 4 through 6 years of age or at least 28 days later
Infants who get one dose of MMR vaccine before their first birthday should get two more doses according to the routinely recommended schedule
Children ≥12 months: Documentation of two doses of MMR vaccine (the first dose of MMR vaccine should be administered at age 12 months or older; the second dose no earlier than 28 days after the first dose)
Teenagers and adults born ≥1957 (no immunity): Documentation of two doses of MMR vaccine, with the second dose administered no earlier than 28 days after the first dose
Post-exposure Prophylaxis
Cannot Readily Show Evidence of Immunity Following Exposure to Measles
Offer post-exposure prophylaxis (PEP) or be excluded from the setting (school, hospital, childcare)
Unvaccinated individuals who receive their first dose of MMR vaccine within 72 hours after exposure may return to childcare, school, or work except healthcare workers
PEP: Administer MMR vaccine within 72 hours of initial measles exposure or immunoglobulin (IG) within six days of exposure
Monitor for signs and symptoms consistent with measles for at least one incubation period following PEP
Note: “Do not administer MMR vaccine and IG simultaneously, as this practice invalidates the vaccine”
MMR vaccine for PEP
Should still offer MMR vaccine even if beyond 72 hours to protect from future exposures
Outbreak control measure for infants <12 months of age: Measles vaccination of infants as young as 6 months of age may be used (revaccinate when they are 12 through 15 months old and again when they are 4 through 6 years of age)
Immunoglobulin (IG) for PEP
IG dosing
IGIM dose: 0.5 mL/kg of body weight (maximum dose = 15 mL)
IGIV dose: 400 mg/kg
IG used for high risk populations
Infants younger <12 months
Intramuscular IG (IGIM) for all
However, if 6 through 11 months, MMR vaccine can be given in place of IG, if administered within 72 hours of exposure
Pregnant women without evidence of measles immunity
Intravenous IG (IGIV)
Severely compromised immune systems
Administer IGIV regardless of immunologic or vaccination status
Note: People cannot return to healthcare settings following receipt of IG | For other settings, such as childcare, school, or work “factors such as immune status, intense or prolonged contact, and presence of populations at risk, should be taken into consideration before allowing people to return”
PEP for healthcare personnel
MMR vaccine should be given within 72 hours or IG should be given within 6 days
“Exclude healthcare personnel without evidence of immunity from duty from day 5 after first exposure to day 21 after last exposure, regardless of post-exposure vaccine”
Isolation
Isolate for four days after they develop a rash
Use airborne precautions in healthcare settings
All healthcare staff entering the room should use respiratory protection consistent with airborne infection control precautions (use of an N95 respirator or a respirator with similar effectiveness in preventing airborne transmission)
Use single-patient airborne infection isolation room (AIIR) for patient with measles
People without evidence of immunity who have been exempted from measles vaccination for medical, religious and now PEP within appropriate timeframe
Exclude from affected institutions in the outbreak area until 21 days after the onset of rash in the last case of measles
Treatment
There is no specific antiviral therapy for measles
Supportive care to address symptoms and complications
Severe measles in children: Administer Vitamin A (a substrate for preserving epithelial cell integrity and involved in immune modulation) immediately on diagnosis and repeated the next day with following dosing
<6 months: 50,000 IU
6–11 months: 100,000 IU
≥12 months: 200,000 IU
Measles and Pregnancy
Pregnant women are considered a ‘high risk’ category due to increased risk for adverse maternal, fetal and newborn events
Maternal: Increased risk of hospitalization and severe respiratory complications including pneumonia
The appropriate use of antenatal corticosteroids improves neonatal outcomes, including decreased severity and/or frequency of respiratory distress syndrome (RDS), intracranial hemorrhage, necrotizing enterocolitis and death. Antenatal corticosteroids, when appropriate, are administered in a clinical setting where patients are at risk for preterm delivery within 7 days, irrespective of membrane status and fetal number.
Clinical Actions:
Risk of preterm delivery within 7 days
Between 24w0d to 33w6d – ‘Recommended’
Single course of corticosteroids
Between 22w0d and 23w6d – ‘May be Considered’
23w0d to 23w6d
Single course of corticosteroids
22w0d to 22w6d
Single course of corticosteroids
Note: ACOG and SMFM revised recommendation states
Antenatal corticosteroids may be considered at 22 0/7 weeks to 22 6/7 weeks of gestation if neonatal resuscitation is planned and after appropriate counseling
Some families may choose to forgo resuscitation and support after appropriate counseling
Between 20w0d and 21w6d – ‘Not Recommended’
Antenatal corticosteroids are not recommended due to lack of data suggesting benefit
Late preterm (34w0d – 36w6d)
ACOG
If no previous corticosteroids
Single course of betamethasone
Not indicated in women diagnosed with clinical chorioamnionitis
SMFM
Single course of betamethasone in specific populations
Population included in ALPS trial: Recommended
Nonanomalous singleton gestation
High risk for preterm delivery (medically indicated or spontaneous)
No prior antenatal steroids
Select populations not in the original ALPS trial: Suggest consideration for use in the following clinical scenarios
Multiple gestations reduced to a singleton gestation ≥14w0d
Fetal anomalies
Expected to deliver in less than 12 hours
Low likelihood of delivery <37 weeks: Recommend against
Pregestational diabetes: Recommend against due to risk for worsening neonatal hypoglycemia
Repeat or Rescue Courses
Regularly scheduled repeat courses or serial (> 2) courses
Not recommended
If a patient has received one prior course of corticosteroids > 14 days ago, is less than 34w0d gestation and is at risk of preterm delivery within 7 days
a single repeat course of corticosteroids should be considered (change from previous ‘may’)
Rescue course corticosteroids could be provided as early as 7 days from the prior dose, if indicated by the clinical scenario (based on Cochrane meta-analysis)
Preterm prelabor rupture of membranes (PPROM)
There is insufficient evidence to make a recommendation for or against repeat or rescue courses
Dose and Regimen: give first dose even if 2nd dose unlikely
Postpartum Hemorrhage – Medications to Treat Uterine Atony
ACOG defines PPH as cumulative blood loss ≥ 1,000 mL or blood loss accompanied by signs or symptoms of hypovolemia within 24 hours after the birth process (including intrapartum) regardless of route of delivery. Unfortunately, postpartum hemorrhage (PPH) is still a leading cause of maternal mortality worldwide. Following this summary, you can find excellent professional resources at the California Maternal Quality Care Collaborative (CMQCC) and ACOG Safe Motherhood Initiative sites.
CLINICAL ACTIONS:
In the setting of PPH, consider the 4 ‘T’s
Tone (atony)
Trauma (laceration)
Tissue (retained products)
Thrombin (coagulopathy)
Uterine atony is the single most common cause of PPH (70-80%)
250 micrograms IM (may repeat in q15 – 90 minutes, maximum 8 doses)
OR
Intramyometrial: 250 micrograms
Avoid: Asthma
Caution: Hypertension, Active Hepatic, Pulmonary, Cardiac Disease
Misoprostol (Cytotec)
600 – 1000 micrograms PR, PO or SL
Hypersensitivity to this medication
NOTE: Contraindications include hypersensitivity to the specific medication
More on Tranexamic Acid (TXA)
ACOG Update
In the WOMAN trial (see Related OBG Topics below) women with PPH received
1 g in 10 mL (100 mg/mL) of tranexamic acid intravenously at a rate of 1 mL per min (i.e., over 10 min)
If bleeding continued after 30 min or stopped and restarted within 24 h of the first dose, a second dose of 1 g of tranexamic acid could be given
Tranexamic acid, administered within 3 hours of birth, has been shown to significantly reduce maternal death due to PPH by approximately 30%
Based on improved outcomes and lack of adverse events including thromboembolism, ACOG has updated the practice bulletin to include the following
Although the generalizability of the WOMAN trial and the degree of effect in the United States is uncertain, given the mortality reduction findings, tranexamic acid should be considered in the setting of obstetric hemorrhage when initial medical therapy fails. (Level B evidence)
World Health Organization Update
Based on evidence review, WHO also supports the use of tranexamic acid with postpartum hemorrhage
Early use of intravenous tranexamic acid (within 3 hours of birth) in addition to standard care is recommended for women with clinically diagnosed postpartum haemorrhage following vaginal birth or caesarean section (Strong recommendation, moderate quality of evidence)
Administration of TXA should be considered as part of the standard PPH treatment package and be administered as soon as possible after onset of bleeding and within 3 hours of birth
The reference point for the start of the 3-hour window for starting TXA administration is time of birth
If time of birth is unknown, the best estimate of time of birth should be used as the reference point
TXA should be used in all cases of PPH, regardless of whether the bleeding is due to genital tract trauma or other causes
SYNOPSIS:
The key to managing PPH is identifying the severity of the situation early and quantifying estimated blood loss (EBL). A second large bore (16 gauge or larger) should be placed and Ringers Lactate used to replace blood loss at 2:1 while, simultaneously as the team is notified, medications are administered to the patient and massive transfusion protocol is initiated. Initiate fundal massage and place a Foley catheter.
KEY POINTS:
ABCs
Airway: Assess and stabilize
Breathing: Supplemental oxygen, 5-7 L/min by tight face mask
Consider intrauterine balloon tamponade or compression sutures for refractory atony
Hospitals and facilities that provide obstetrical services should have uterine balloon tamponade and vacuum-induced hemorrhage-control devices available to the care team in case of PPH
Surgical Interventions may be a life-saving measure and should not be delayed while waiting to correct coagulopathy
Quantitative measurement of blood loss is more accurate than visual estimation (see ‘Learn More – Primary Sources’ below) and require 2 key elements
Direct measurement of blood loss
Protocols for collecting and reporting a cumulative record of blood loss following delivery
Note: The FDA, the World Health Organization, and other professional bodies have released an alert following drug-error deaths related to TXA | TXA use during cesarean delivery has been associated with fatal accidental intrathecal administration because the ampoules of local anesthetic and tranexamic acid are similar in appearance | TXA should not be stored on or near an anesthetic trolley
While historically oxygen has routinely been used on labor floor in the presence of category II and III tracings, current guidance recommends against this practice. The evidence, particularly a key paper by Raghuraman et al. does not demonstrate any benefit.
Maternal Oxygen Supplementation Compared With Room Air for Intrauterine Resuscitation (JAMA Pediatrics)
Background
The research team assessed whether there was an association between umbilical artery (UA) gas measures and neonatal outcomes with peripartum maternal oxygen administration vs room air
Methods
Systematic review and meta-analysis
Study inclusion criteria
RCTs
Studies that compared oxygen with room air at the time of scheduled cesarean delivery or labor
Participants were patients with singleton, nonanomalous pregnancies
Primary outcome
Umbilical artery (UA) pH
Secondary outcomes
UA pH <7.2 | UA PaO2 | UA base excess | Apgar scores (1 and 5 min) | NICU
Conclusion
Supplemental oxygen therapy at delivery was not associated with improvement in umbilical artery pH or other neonatal outcomes
KEY POINTS:
An associated editorial to the above study concludes
While maternal oxygen administration to the normally oxygenated mother in labor is likely as innocuous as it is useless, concern for the practice of evidence-based medicine would seem to suggest that recommendations for its use in 2 million to 3 million women annually may be inappropriate
ACOG states
ACOG recommends against routine maternal oxygen administration for category II or III fetal heart rate tracings in the absence of maternal hypoxia
Thyroid disease, both thyrotoxicosis and hypothyroidism, are associated with adverse pregnancy outcomes and poor fetal development, including neurocognitive outcomes. Given the importance of understanding physiology, changes during pregnancy, and management, ACOG has published recommendations to guide clinical decision-making. Universal TSH screening for thyroid disease in pregnancy is not recommended. Continue risk-based testing, using updated risk factors (autoimmune disease, infertility/recurrent miscarriage, prior thyroid disease, medications, recognizing these identify most but not all cases Subclinical thyroid disease (abnormal TSH but normal free T4) may require treatment but only if identified in the first trimester. However, overt hyperthyroidism and hypothyroidism warrant further management
Maternal thyroid volume increases 10% to 30% in pregnancy, especially in 3rd trimester, as a result of increased blood volume and extracellular fluid
An enlarged thyroid gland in isolation is not an indication for screening for thyroid disease if no other clinically relevant history, symptoms, or signs are present
TSH (thyroid stimulating hormone, or ‘thyrotropin’)
Decreased in early pregnancy
β-hCG weakly stimulates TSH receptors causing increased T4 (thyroxine) levels | Estrogen stimulates higher levels of thyroid-binding globulin that transport thyroid hormone in the blood
American Thyroid Association recommends the following in the late first trimester if local reference ranges for TSH are unavailable: Reduce lower reference range by 0.4mU/L | Reduce upper reference range by 0.5mU/L | If trimester- and lab-specific ranges unavailable, a practical reference range of ~0.1 to 4.0 mU/L in early pregnancy may be used
After first trimester: Use non-pregnant reference ranges as TSH increases due to increased production of placental deiodinase
Maternal transfer of T4 to fetus
Necessary for fetal brain development
30% of umbilical cord T4 is maternally derived
Maternal iodine requirements
Pregnant women: Approximately 250 micrograms
Lactating women: 150 micrograms
Majority of women in US have sufficient intake
Workup of Thyroid Abnormalities (Clinically Indicated Testing)
Test TSH first
TSH high or low (abnormal): Reflex to free T4 (plus total T3 for hyperthyroidism)
Free T4 is normal: Thyroid disease is subclinical
Anti-thyroid peroxidase antibodies
Testing for these anti-bodies (without history and normal thyroid tests) does not improve pregnancy outcomes, therefore is not recommended
TPOAb testing may be used selectively (e.g., infertility, recurrent miscarriage, autoimmune disease risk)
Euthyroid TPOAb-positive patients should not be treated with levothyroxine (strong recommendation)
Hyperthyroidism
Low TSH and Increased free T4
Universal screening not recommended | Diagnosis based on clinical symptoms | 95% will be due to Graves disease
Graves ophthalmopathy: Upper eyelid retraction | Edema | Erythema of the periorbital tissues and conjunctivae | Proptosis (see ‘Learn More, Primary Sources’ for additional reference including pictures)
Dermopathy: For example pretibial myxedema
Potential outcomes if left untreated
Iatrogenic preterm deliveries | LBW | Stillbirth
Fetal thyrotoxicosis
Caution: Not necessarily related maternal clinical thyroid status
Treatment: Follow free T4 and total T3 every 2 to 4 weeks until titrated to high normal range
First trimester
PTU: 100 to 600mg divided TID
After first trimester
PTU: 100 to 600mg divided TID or
Methimazole 5 to 30mg divided into BID
Adverse events
Do not use methimazole in first trimester due to association with birth defects including esophageal/choanal atresia and aplasia cutis
Due to (rare) association of PTU with hepatotoxicity, option to transition to methimazole or continue PTU after first trimester
Both PTU and methimazole have risk of leukopenia (10% patients) but does not require therapy termination
Agranulocytosis: Rare side effect | Remain alert for sore throat or fever which does require CBC and cessation of medication
Symptom control: Propranolol 10 to 40mg TID/QID
Subclinical hyperthyroidism and gestational transient thyrotoxicosis
Do not require antithyroid drugs
Use beta-blockers only for symptoms
Note: Maternal antibodies found in Graves disease cross the placenta and are cleared slowly | Notify neonatology of maternal diagnosis as neonatal Graves disease may not present immediately following delivery
Hypothyroidism
High TSH, Low Free T4
Diagnosis based on history (personal or family), clinical symptoms or type 1 diabetes, other autoimmune disorders
Symptoms
Cold intolerance | Muscle cramps | Weight gain | Edema | Dry skin | Hair loss
Prolonged relaxation of deep tendon reflexes is a notable feature
Cardiac myopathy leading to heart failure and pulmonary hypertension | More common in pregnancy | Reversible if treated
Other clinical associations
Preeclampsia | Anemia |Sepsis
Treatment
PTU: 1,000mg loading PO then 200mg q6 hours
Iodine: Initiate 1 to 2 hours after PTU via sodium iodide (500-1,000mg IV q8h) or potassium iodide (5 drops by mouth q8 hours) or lugol solution (10 drops by mouth q8h) or lithium carbonate (iodine anaphylaxis history, 300mg PO q6h)
Dexamethasone: 2mg IV q6h x4 doses or hydrocortisone 100mg IV q8h x3 doses
Propranolol, labetalol, and esmolol
Have been used to treat tachycardia, but caution warranted in setting of heart failure
Postpartum Thyroiditis
Thyroid dysfunction within 12 months of delivery
Diagnosis: New-onset abnormal TSH and free T4
First phase
Initially thyrotoxicosis as thyroid gland is destroyed and T4 released
Mild symptoms controlled with beta-blockers rather than PTU or methimazole
Second phase (4 to 8 months postpartum)
Overt hypothyroidism with typical symptoms and thyromegaly
Depression
Order TSH screen for new onset postpartum depression or any new diagnosis of depression
Risk of permanent overt hypothyroidism
Majority of cases will spontaneously resolve
Approximately a third will not resolve (highest risk associated with higher antibody titers)
High risk of permanent hypothyroidism (~30%) requires follow-up
Thyroid Nodules Detected During Pregnancy
Prevalence: 1% to 2% | 90% to 95% of solitary nodules are benign
Aside from history and physical examination, order
TSH
Neck ultrasound
Radioiodine scanning not recommended due to theoretical risk with fetal irradiation
However, if patient inadvertently receives radioiodine in the first trimester, risk of fetal thyroid damage low because fetal thyroid is not active until after the first trimester
If cancer identified
Surgical treatment in first and second trimesters with thyroidectomy “may be performed” but usually delayed to avoid possible damage to parathyroid glands
Management is multidisciplinary and should include possibility of familial cancer syndrome (uncommon)
Chronic Hypertension in Pregnancy: Evaluation and Management
CLINICAL ACTIONS:
ACOG has released recommendations on chronic hypertension in pregnancy. Management of chronic hypertension in pregnancy depends on gestational age and symptoms. Initial assessment, including identification of end-organ damage and evaluation of medications will drive treatment and delivery planning.
Ideally preconception or the first prenatal visit is the optimal time to establish a diagnosis (primary vs. secondary hypertension) and assess for end-organ damage, based on a thorough history and physical
Laboratory tests
Complete blood count
Liver function tests
Serum electrolytes (esp. potassium)
Renal Function Tests
Serum creatinine
Mild renal impairment: Cr 0.9-1.4
Moderate renal impairment: Cr 1.4-2.4
Severe renal impairment: Cr 2.4-2.8
Blood urea nitrogen
Spot urine protein/creatinine to screen for proteinuria
<0.15 denotes patient spilling <300 mg for a 24-hour sample
If spot urine ratio elevated, do 24-hour urine
Note: 24-hour urine assessment not required if normal Cr and spot urine ratio <0.15
Order ECG if ≥1 of the following
Chronic hypertension present >4 years
Maternal age >30 years with long standing hypertension
The benefits of treating mild to moderate chronic hypertension in pregnancy are not clear, thus a conversation with patients (i.e. shared decision-making) is warranted. Timing of delivery depends on severity of disease and gestational age. Women with chronic hypertension remain at risk for complications during the postpartum period so early follow-up is recommended.
KEY POINTS:
Medical Management
Choice of Antihypertensive
Most commonly used antihypertensives
Labetalol – ‘preferred’: 200 to 2,400 mg/d po (2 to 3 divided doses)
Initiate at 100 to 200 mg twice a day
Watch for potential bronchospasm
Avoid in women with asthma, heart disease, congestive heart failure, bradycardia and heart block
Nifedipine – ‘preferred’: 30 to 120 mg/d po (avoid sublingual)
Initiate at 30 to 60 mg daily (extended release)
Avoid in women with tachycardia
Methyldopa – ‘less favored’: 500 to 3,000 mg/d po (2 to 4 divided doses)
Initiate at 250 mg twice or 3 times/day
May not be as effective and limited by side-effects such as dizziness, depression or sedation
Second line therapy
HCTZ (considered a safe diuretic)
Other medications are available and may be used with MFM consultation
Note: The following medications are not recommended
Ace inhibitors | Angiotensin II receptor blockers | Renin inhibitors | Mineralocorticoid receptor antagonists | Atenolol (due to risk for FGR and LBW)
Threshold for Initiation of therapy
Based on the CHAP Trial (see ‘Related ObG Entries’ below), ACOG and SMFM have revised guidance regarding initiation of therapy for women with mild chronic hypertension during pregnancy
Start antihypertensive therapy at >140/90
Patient on medications prior to pregnancy
In the absence of mitigating factors or side effects
Maintain on their medications
Do not discontinue and wait until blood pressures in the severe range to initiate therapy
Individualize decision whether to discontinue
Replace contraindicated medications and monitor therapy and BP targets accordingly
Target BP
ACOG
Notes that RCT (CHAP Trial) demonstrated benefit of using 140/90 as threshold but did not determine ideal target BP or if there is a BP at which growth restriction may be a concern
SMFM
“…recommends treatment with antihypertensive therapy for mild chronic hypertension in pregnancy to a goal BP <140/90 mm Hg”
Aspirin
Use aspirin for risk reduction (see ‘Related ObG Topics below)
Initiate daily low dose aspirin (81 mg) between 12 to 28 weeks gestation
Fetal Surveillance
Antepartum
Timing/interval of testing not well established
Assess fetal growth in the 3rd trimester
Intrapartum
Continuous fetal monitoring
Timing of Delivery
Chronic HTN and no medications
Delivery <38w0d not recommended
Chronic HTN well controlled on maintenance antihypertensive medication
Delivery <37w0d not recommended
Chronic HTN with superimposed preeclampsia without severe features
Expectant management with delivery at 37w0d
Chronic HTN with superimposed preeclampsia with severe features
Expectant management under certain circumstances until delivery at 34w0d (inpatient care only)
Initiation of antenatal steroids as per guidelines (see ‘Related ObG Topics below)
Note: When considering the latest time to deliver, ACOG states
…expectant management beyond 39 0/7 weeks of gestation should only be done after careful consideration of the risks and benefits and with appropriate surveillance
Postpartum
Early ambulatory visits (within 2 weeks) postpartum
Severe HTN or superimposed preeclampsia may develop for the first time in the postpartum period
Patient may return to prepregnancy regimen and managed appropriately, without fetal considerations
Note: Avoid methyldopa in postpartum period due to risk for depression
Careful medication titration to achieve BP no higher than 150/100 mm Hg
Analgesia
NSAIDs were not associated with BP elevation based on data from women with preeclampsia with severe features
Breastfeeding
Antihypertensives can be used in breastfeeding women
Propranolol and labetalol are preferred due to lower levels in breast milk compared to some other medications
ACE inhibitors can also be used safely unless high doses required
Calcium channel blockers are not associated with adverse outcomes
Note: Diuretics may reduce quantity of breast milk
ISUOG Recommendations for Preeclampsia Prevention: Combined Screening and the Role of Ultrasound
SUMMARY:
The ISUOG Clinical Standards Committee, based on the latest evidence, has released practice guidelines that provide recommendations regarding the role of ultrasound in screening for and follow-up of preeclampsia. Preventative strategies (such as low-dose aspirin) for preeclampsia are effective if started in the first trimester and should begin as soon as high-risk status is identified.
Given the superiority of combined screening, the use of Doppler cut-offs as a standalone screening modality should be avoided if combined screening is available (GRADE OF RECOMMENDATION: B)
Note: Screening refers to identification of at risk cases that may lead to prevention | Prediction refers to ability to identify at risk cases, but no evidence available regarding improved outcomes
Combined Screening (10-13 weeks) – Preferred where available
ASPRE trial results with a 10% FPR (see ASPRE summary in ‘Related ObG Topics’ below)
100% detection rate for preeclampsia <32 weeks
75% detection rate for preeclampsia <37 weeks
43% detection rate for preeclampsia ≥37 weeks
Combined screening approach is preferred over ultrasound alone and includes the following (see summary of ASPRE algorithm details in ‘Related ObG Topics’ below)
Maternal factors
History | Demographics | CVD and metabolic profile
Maternal arterial BP
Placental growth factor (PlGF)
Pulsatility index (PI) should be used to assess uterine artery resistance
Transabdominal approach preferred as used for most studies
Transabdominal: Use color flow mapping on a mid-sagittal view of the uterus at the level of the cervical internal os (transabdominal approach)
Transvaginal: Also obtain mid-sagittal view of the uterus, with lateral movement until paracervical vascular plexus is seen and uterine artery is also at the level of the internal cervical os
Identify an ascending or descending branch of the uterine arteries
Narrow Doppler sampling gate (2 mm)
Insonation angle <30 degrees
Peak systolic velocity of a uterine artery should be greater than 60 cm/s
PI measurement obtained when 3 identical waveforms are captured
95th percentile uterine artery mean PI (11-13 weeks)
Transabdominal: 2.35
Transvaginal 3.10 for CRL up to 65 mm
Uterine artery PI may be affected by
Ethnicity: African origin has higher PI
Obesity: Decreasing PI with increasing BMI
History of preeclampsia: Increased PI
Note: Placental volume and vascularization indices are not recommended | Combined screening in the second trimester compares favorably to first trimester, but aspirin intervention is ineffective if initiated >20 weeks
Ultrasound Screening Only
First Trimester Ultrasound Screening (10-13 weeks)
Due to maternal effects and lesser performance, uterine artery PI is not preferred as a stand-alone test based on cut-offs, but should preferably be incorporated into a combined, multifactorial screening model (see above)
Uterine artery PI >90th percentile in the first trimester detects
47.8% of women who will develop early PE (7.9% FPR)
26.4% of women who will develop any PE (6.6% FPR)
PI is superior to resistance index (RI) or uterine artery notching as a preeclampsia predictive tool
PI is more stable than RI, and may still be used in cases of absent or reversed diastolic values
Uterine artery notching is a subjective measure with low specificity
Associated with 22-fold increased risk for preeclampsia and 9-fold increased risk for an SGA neonate
However, may be observed in up to 50% of patients at 11-13th weeks
Second Trimester Ultrasound Screening
Uterine artery PI may be performed at time of the second trimester scan (10% FPR)
85% detection of early-onset preeclampsia
48% detection of late-onset preeclampsia
95th percentile uterine artery mean PI (23 weeks)
Transabdominal: 1.44
Transvaginal: 1.58
Third Trimester Ultrasound Screening
Use of PI during this period is not recommended due to insufficient outcomes data
Multifetal Pregnancies
Use twin-specific reference ranges
Increased placental mass and lower mean uterine artery resistance seen in multiple gestation
Fetal Alcohol Spectrum Disorders – CDC Summary and Updates
WHAT IS IT?
The current understanding of Fetal Alcohol Spectrum Disorder (FASD) is that there is no known safe amount of alcohol during pregnancy or when trying to get pregnant. All types of alcohol are equally harmful, including all wines and beer. Professional colleges recommend screening women in pregnancy. Fetal Alcohol Syndrome (FAS) is on the most severe end of the spectrum.
Smooth philtrum (ridge between nose and upper lip)
Thin vermillion (upper lip)
Small palpebral fissures (distance between inner and outer corners of the eyes) giving the eyes a wide-spaced appearance
Growth problems (prenatal or postnatal)
Height and/or weight ≤10th percentile
CNS
Structural
Head circumference ≤10th percentile
Clinically significant brain abnormalities observable through imaging
Neurological deficits unrelated to a postnatal insult or fever
Functional Performance below expectations
Global cognitive or intellectual deficits (Low IQ or developmental delay in younger children) or
Problems in at least 3 of the following areas
Cognitive or developmental deficits or discrepancies | Executive functioning deficits | Motor functioning delays | Attention deficit or hyperactivity | Social skills | Other problems such as sensory / language / memory
Maternal Alcohol Exposure
Helpful if maternal alcohol use can be confirmed during pregnancy
Confirmation of maternal alcohol use is not needed if child meets the other, above criteria
CNS, cognitive and behavioral effects without growth restriction and typical facial experience
Intellectual disabilities | Behavior and Learning abnormalities
Difficulties with math, memory, attention, judgment and impulse control
Requires confirmation of prenatal alcohol exposure
Alcohol-Related Birth Defects (ARBD)
Abnormal physical findings only (see more detail below in ‘Key Points’)
Heart | Kidneys | Bones | Hearing
Requires confirmation of prenatal alcohol exposure
Neurobehavioral Disorder Associated with Prenatal Alcohol Exposure (ND-PAE)
ND-PAE was first included as a recognized condition in the Diagnostic and Statistical Manual 5 (DSM 5) of the American Psychiatric Association (APA) in 2013
Problems identified
Thinking and memory, where the child may have trouble planning or may forget material he or she has already learned
Behavior problems, such as severe tantrums, mood issues (for example, irritability), and difficulty shifting attention from one task to another
Trouble with day-to-day living, which can include problems with bathing, dressing for the weather, and playing with other children.
Diagnosis requires
>13 alcoholic drinks per month (30-day period) of pregnancy or
> 2 alcoholic drinks in one sitting
KEY POINTS:
Structural abnormalities associated with prenatal alcohol exposure include
Facial abnormalities (described above plus short nose, cleft lip/palate)
Cardiac anomalies (ASD, VSD, abnormal great vessels)
Guidance Update: Diagnosis and Management of PROM (Prelabor Rupture of Membranes)
SUMMARY:
ACOG guidance on Prelabor Rupture of Membranes (PROM) addresses current literature especially related to management of late preterm PROM (34w0d to 36w6d). Following appropriate counseling, expectant management or delivery is appropriate. The use of ‘prelabor’ is in keeping with reVITALize terminology (see ‘Related ObG Topics’ below) and is defined as the ‘spontaneous rupture of membranes that occurs before the onset of labor’.
It is critically important that patients are counseled on the higher rates of morbidity associated with expectant management, which may be greater than previously reported, to ensure they can make a fully informed decision regarding their care
Latency
40-50% will deliver within 1 week and 70-80% will deliver within 2-5 weeks
Pulmonary hypoplasia
Will occur in approximately 10-20% of cases
Insufficient data to recommend ultrasound for determination of lung volumes or function
Oligohydramnios can result in Potter’s deformation sequence
IV ampicillin [2 g every 6 hours] and erythromycin [250 mg every 6 hours] for 48 hours followed by oral amoxicillin [250 mg every 8 hours] and erythromycin base [333 mg every 8 hours] for an additional 5 days (7 days total)
Azithromycin (e.g., 1 g single dose) “is a suitable alternative” to replace erythromycin if unavailable or poorly tolerated
Amoxicillin–clavulanic acid
Not recommended due to increased risk for necrotizing enterocolitis
Allergy to β-lactam antibiotics
“May be reasonable to consider another agent against GBS” | Choice based on severity of allergic reaction and susceptibility profiling
Unclear as to whether cerclage should be removed or retained but if retained, antibiotic therapy should not be extended beyond 7 days
Note: There are multiple regimens in use | There is no evidence to support a single optimal regimen for latency antibiotics
Patients with PROM before 32w0d and imminent delivery are candidates for fetal neuroprotective treatment with magnesium sulfate (if no contraindications)
Obtain vaginal/rectal swab for GBS | Administer GBS prophylaxis as indicated
HSV infection and Preterm PROM
Risk of vertical transmission is 30-50% with primary HSV and 3% with recurrent HSV
Recurrent active HSV
Expectant management is recommended <34w0d
Initiate HSV therapy
Corticosteroids | Antibiotics | Magnesium sulfate per indications
Cesarean section is indicated if active disease or prodromal symptoms are present at time of delivery
Primary HSV
Management less clear due to high risk of vertical transmission
HSV therapy is recommended
Cesarean delivery recommended if active lesions are present
HIV infection and Preterm PROM
Optimal management is uncertain due to concern of vertical transmission with PROM
Management should include a physician with expertise in the management of HIV in pregnancy and standard HIV guidelines should be followed
Most recent data suggest that vertical transmission risk my not be increased if the patient is on highly active antiretroviral therapy with a low viral load and has received antepartum and intrapartum zidovudine
Management should be individualized
If gestational age is early, but patient is on appropriate therapy with a low viral load expectant management may be appropriate
Late Preterm (34w0d to 36w6d)
“Either expectant management or immediate delivery is a reasonable option”
Data suggests when comparing these 2 options
No difference in neonatal sepsis
Newborn: Increased respiratory distress, mechanical ventilation, ICU stay in the immediate group
Maternal: Increased hemorrhage and infection in expectant management group
Administer single-course corticosteroids if
Not previously given
Delivery expected in >24 hours and ≤7 days
No chorioamnionitis
Screen for GBS and administer prophylaxis as indicated
Chorioamnionitis: Treat and plan for delivery
ACOG states (PB 831)
Care should be individualized through shred decision making, and expectant management should not extend beyond 37 0/7 weeks of gestation
Outside the scenario of unknown GBS status, latency antibiotics are not appropriate in this setting
Term (≥37w0d)
Induction is recommended vs expectant management | Short period of expectant management (12 to 24 hours) “may be appropriately offered”
If no spontaneous labor, induce labor with oxytocin
Allow adequate time (12-18 hours) for latent phase to progress before performing a cesarean section for failed induction of labor
Induction with prostaglandins equally as effective as oxytocin but may have higher rates of chorioamnionitis
Insufficient data to recommend for or against cervical ripening with mechanical methods such as a Foley balloon
Insufficient evidence to recommend antibiotic prophylaxis beyond GBS indications
If a patient declines delivery and requests expectant management, counsel regarding risks and benefits
If fetal and maternal status are reassuring, expectant management ‘may be acceptable’
Screen for GBS and administer prophylaxis as indicated
Chorioamnionitis: Treat and plan for delivery
Key Points:
PROM-Related Risks
Preterm birth
50% of patients will deliver within 1 week
Risks associate with prematurity include RDS, sepsis, IVH and NEC
Infection
Preterm PROM and intrauterine inflammation are associated with increased risk of neurologic injury
Intraamniotic infection (15-25%)
Postpartum infection (15-20%)
Abruption (2-5%)
Infection and umbilical cord accidents are associated with a 1 to 2% chance for fetal demise
Additional Clinical Considerations
Membranes may reseal spontaneously leading to good outcomes
Hospital admission is recommended if the fetus is viable to monitor for signs of infection, abruption and fetal compromise
Acceptable strategy includes periodic ultrasound for fetal growth and FH monitoring (precise timing not established)
No clinical utility evidence for the use of serial WBC counts or other infectious markers
Use of tocolysis
Tocolytic therapy is not recommended at 34w0d to 36w7d gestation
Can be considered for steroid benefit at earlier gestational age and during maternal transport
GBS as per standard protocol
GBS prophylaxis should be given based on prior culture results or intrapartum risk factors if cultures not performed or unavailable
PROM Following Amniocentesis
Risk of PROM following amniocentesis is 1%
Outpatient, expectant management
Monitor regularly with ultrasound and counsel patients to watch for signs of infection, bleeding and/or miscarriage
Contrary to spontaneous PROM, good outcomes have been reported
AF fluid reaccumulated within 1 month in 72% of patients
Perinatal survival rate was 91%
Preterm PROM and Future Pregnancies
Increased risk of recurrent PROM and preterm birth
Offer progesterone supplementation starting at 16-24 weeks
OBG Project CME requires a modern web browser (Internet Explorer 10+, Mozilla Firefox, Apple Safari, Google Chrome, Microsoft Edge). Certain educational activities may require additional software to view multimedia, presentation, or printable versions of their content. These activities will be marked as such and will provide links to the required software. That software may be: Adobe Flash, Apple QuickTime, Adobe Acrobat, Microsoft PowerPoint, Windows Media Player, or Real Networks Real One Player.
Disclosure of Unlabeled Use
This educational activity may contain discussion of published and/or investigational uses of agents that are not indicated by the FDA. The planners of this activity do not recommend the use of any agent outside of the labeled indications.
The opinions expressed in the educational activity are those of the faculty and do not necessarily represent the views of the planners. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications, and warnings.
Disclaimer
Participants have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional development. The information
presented in this activity is not meant to serve as a guideline for patient management. Any procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this activity should not be used by clinicians without evaluation of their patient’s conditions and possible contraindications and/or dangers in use, review of any applicable manufacturer’s product information, and comparison with recommendations of other authorities.
Jointly provided by
NOT ENOUGH CME HOURS
It appears you don't have enough CME Hours to take this Post-Test. We no longer offer Hours.
Leaving ObG Website
You are now leaving the ObG website and on your way to PRIORITY at UCSF, an independent website. Therefore, we are not responsible for the content or availability of this site